- info@careermakers.edu.np
- +977 1 4423870
Atorlip-20
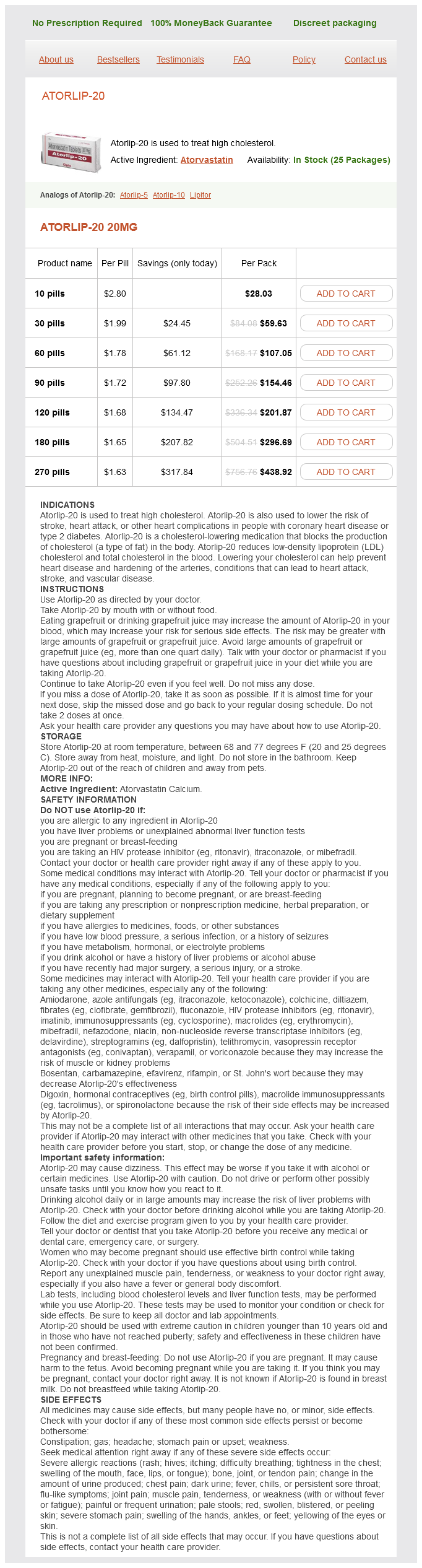
Atorlip-20 20mg
- 10 pills - $28.03
- 30 pills - $59.63
- 60 pills - $107.05
- 90 pills - $154.46
- 120 pills - $201.87
- 180 pills - $296.69
- 270 pills - $438.92
Atorlip-20 dosages: 20 mg
Atorlip-20 packs: 10 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills
In stock: 661
Only $1.73 per item
Description
Postplacental or delayed levonorgestrel intrauterine device insertion and breast-feeding duration sitosterol cholesterol ratio generic atorlip-20 20 mg with mastercard. Lactogenesis after early postpartum use of the contraceptive implant: A randomized controlled trial. Immediate postpartum initiation of etonogestrel-releasing implant: A randomized controlled trial on breastfeeding impact. Puerperal septic pelvic thrombophlebitis: Incidence and response to heparin therapy. Prophylactic antibiotics for the prevention of postpartum infectious morbidity in women infected with human immunode ciency virus: A randomized controlled trial. Increased risk of endometritis and wound infection after cesarean section in insulin-dependent diabetic women. Polymicrobial early postpartum endometritis with facultative and anaerobic bacteria, genital mycoplasmas, and chlamydia trachomatis: Treatment with piperacillin or cefoxitin. Oral and intramuscular treatment options for early postpartum endometritis in low-resource settings: A systematic review. Obesity as an independent risk factor for infectious morbidity in patients who undergo cesarean delivery. Maternal peripartum complications associated with vaginal group B streptococci colonization. Vaginal colonization with group B beta-hemolytic streptococcus as a risk factor for post-cesarean section febrile morbidity. Vaginal preparation with antiseptic solution before cesarean section for preventing postoperative infections. Randomized clinical trial of extended spectrum antibiotic prophylaxis with coverage for Ureaplasma urealyticum to reduce post-cesarean delivery endometritis. Gentamicin and clindamycin therapy in postpartum endometritis: the ef cacy of daily dosing versus dosing every 8 hours. Prevena, negative pressure wound therapy applied to closed Pfannenstiel incisions at time of caesarean section in patients deemed at high risk for wound infection. Wound dehiscence: Secondary closure with suture versus noninvasive adhesive bandage. A randomized trial of secondary closure of super cial wound dehiscence by surgical tape or suture. A prospective randomized evaluation of negative-pressure wound dressings for diabetic foot wounds.
Green Olive (Olive). Atorlip-20.
- How does Olive work?
- Dosing considerations for Olive.
- Reducing the risk of heart diseases and heart attack.
- Are there any interactions with medications?
- What other names is Olive known by?
- Decreasing the chance of getting serious conditions like breast cancer and colorectal cancer. However, there is no evidence olive oil can help treat these conditions.
- What is Olive?
- Lowering cholesterol in people with high cholesterol levels.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96262
Anemia is usually de ned as a hemoglobin less than 11 g/dL and hematocrit less than 33% in the rst trimester definition de cholesterol hdl buy atorlip-20 20 mg amex, hemoglobin less than 10. Anemia may be caused by decreased production of red blood cells, by increased destruction of red blood cells, or by blood loss. Anemia in pregnancy is complicated by increased iron requirements and an expanded blood volume. Most of these conditions can be ruled out by history, physical exam, and exclusion of underlying diagnoses. These conditions cannot be reliably differentiated with antiplatelet antibody testing or any other diagnostic test. To be classi ed as gestational thrombocytopenia, there are several conditions that must be satis ed. Gestational thrombocytopenia is mild, with platelet counts greater than 70,000/µL. There is no history of signi cant bleeding and no history of thrombocytopenia prior to pregnancy. Platelet counts generally return to normal within 212 weeks following delivery, and there is an extremely low risk of fetal or neonatal thrombocytopenia. Women with gestational thrombocytopenia are not at risk for maternal or fetal hemorrhage or bleeding complications [22]. Less commonly, fetal intracranial hemorrhage may develop, unrelated to mode of delivery. Onset of thrombocytopenia during the third trimester should prompt consideration of gestational hypertensive disorders, which are associated with about 20% of maternal thrombocytopenia, and decreasing platelet count is considered a sign of worsening of disorders of this spectrum (see also Chapter 1 in Maternal-Fetal Evidence Based Guidelines). These disorders are associated with an increase in platelet destruction but the underlying physiology is not known. Platelet function may be reduced even if platelet counts are normal, and thrombocytopenia may occur prior to other manifestations of gestational hypertension. Neonatal thrombocytopenia following gestational hypertension is increased in premature infants but not in term infants [22]. The overall result is the creation of a hypercoagulable state that is exacerbated by venous stasis and compression of the inferior vena cava and pelvic veins by the enlarging uterus [3,23]. This places the pregnant women at increased risk for such phenomena as deep venous about 25%, resulting in an anemia of dilution, as measured by hemoglobin and hematocrit, that is physiologic in pregnancy. Iron requirements increase in order to support the increase in red blood cell mass, support the requirements of the fetus and placenta, and prepare for blood loss during delivery. Ferritin levels have the highest sensitivity and speci city for iron de ciency, with levels less than 1015 g/dL being diagnostic of iron de ciency [21]. The typical diet contains 15 mg of elemental iron per day, while the recommended dietary daily allowance during pregnancy is 27 mg/day [21].
Specifications/Details
Episiotomy There is insuf cient evidence (no trials) to assess the bene ts and risks of episiotomy in operative deliveries cholesterol jama atorlip-20 20 mg purchase otc. Lateral episiotomy has been shown to be protective against anal sphincter injuries in vacuum deliveries, compared with mediolateral and median episiotomies, in a meta-analysis [30]. The number of mediolateral episiotomies needed to prevent one sphincter injury in vacuum extractions was 12, whereas ve mediolateral episiotomies could prevent one sphincter injury in forceps deliveries [31,32]. Episiotomy should not be routinely performed, as it is associated with perineal lacerations in nonoperative vaginal deliveries. Maternal and neonatal effects of outlet forceps delivery compared with spontaneous vaginal delivery in term pregnancies. Vacuum Application Vacuum application, if performed, should begin with low suction and be slowly increased to vacuum of about 0. Compared with stepwise negative pressure for vacuum delivery, rapid negative pressure application is associated with reduced duration (by 6 minutes) of vacuum procedure, but no other maternal or perinatal effects, in a small trial [23]. The risk of cephalohematoma increases as the time of vacuum application increases. A prospective randomized controlled trial of the Kiwi OmniCup versus conventional ventouse cups for vacuum-assisted vaginal delivery. Kiwi OmniCup versus Malmstrom metal cup in vacuum assisted delivery: A randomized comparative trial. Third- and fourth-degree perineal tears among primiparous women in England between 2000 and 2012: Time trends and risk factors. Morbidity experienced by women before and after operative vaginal delivery: Prospective cohort study nested within a two-centre randomised controlled trial of restrictive versus routine use of episiotomy. Evaluation of pelvic oor symptoms and sexual function in primiparous women who underwent operative vaginal delivery versus cesarean delivery for second-stage arrest. Obstetrical anal sphincter laceration and anal incontinence 510 years after childbirth. Randomized clinical trial to assess anal sphincter function following forceps or vacuum assisted vaginal delivery. A randomized comparison of assisted vaginal delivery by obstetric forceps and polyethylene vacuum cup. A randomized prospective trial of the obstetric forceps versus the M-cup vacuum extractor. Risk factors and morbidity associated with suboptimal instrument placement at instrumental delivery: Observational study nested within the instrumental delivery & ultrasound randomised controlled trial. Instrumental delivery and ultrasound: A multicentre randomised controlled trial of ultrasound assessment of the fetal head position versus standard care as an approach to prevent morbidity at instrumental delivery. Morbidity associated with episiotomy in vacuum delivery: A systematic review and meta-analysis.
Syndromes
- Nutritionists or dietitians
- Vocabulary increasing to over 2,000 words
- To ensure your safety, look into buying products such as a gas detector that gives off alarms you can see and hear.
- Liver failure
- Smoking
- Heart bypass surgery
- Your diet
- Clean catch urine collection
- You have symptoms of histoplasmosis, especially if you have a weakened immune system or have been recently exposed to bird or bat droppings
- Try to appear strong, confident, aware, and secure in your surroundings.
Related Products
Additional information:
Usage: gtt.
Tags: buy atorlip-20 20 mg amex, atorlip-20 20 mg order without a prescription, atorlip-20 20 mg order without prescription, 20 mg atorlip-20 order with visa
9 of 10
Votes: 317 votes
Total customer reviews: 317
Customer Reviews
Gamal, 58 years: There was also no difference in the rate of cesarean section or adverse outcomes [133]. Neonatal mortality and morbidity rates in late preterm births compared with births at term. In the past a rigid stainless steel instrument was used, now replaced by disposable equipment. It is this relative ease of application that is rapidly pushing optogenetics into clinical trials in human patients.
Bozep, 27 years: The risk of undergoing either uterine exploration or curettage is 9%18%, and more likely if rupture occurs prior to 20 weeks of gestation. Ultrasound can be used to con rm ndings, and interventions may be offered [21,22]. This allows for histopathological analysis (ability to differentiate between in situ and invasive carcinoma) and immunohistochemical staining for hormone receptors, Her2, and other markers. Treatment of habitual abortion with human chorionic gonadotropin: Results of open and placebo-controlled studies.
Cole, 65 years: Numerous psychological theories have also been proposed to explain the phenomenon of nausea and vomiting in pregnancy. The barrier methods require personal skill regarding correct placement and insertion of the devices in addition to the commitment to regular consistent use. Whether the sex of the fetus should be revealed to the patient with a singleton gestation should be addressed. An induction based solely on maternal request should be designated as such (induction for maternal request).
Kippler, 34 years: Dual color neural activation and behavior control with Chrimson and CoChR in Caenorhabditis elegans. The general intervention with the partogram is early use of oxytocin as soon as the cervical dilatation falls to the right of the partogram, usually on the 2-hour cervical examinations. Postoperative care Remove dressing and irrigate at 24h, can then be followed up in community if tolerating dressing changes. If there is decreased input from the cerebral hemi spheres, decreased input through the cortical spinal tract, a functioning rubrospinal tract, and motor flexor of the distal limb, inhibition of extensor muscles becomes dominant, resulting in decorticate activity.