- info@careermakers.edu.np
- +977 1 4423870
Fosamax
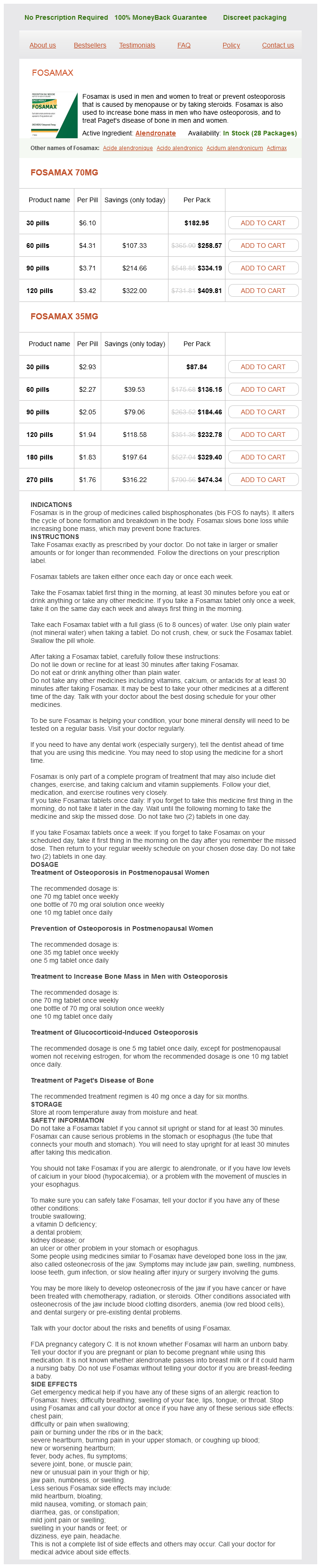
Fosamax 70mg
- 30 pills - $182.95
- 60 pills - $258.57
- 90 pills - $334.19
- 120 pills - $409.81
Fosamax 35mg
- 30 pills - $87.84
- 60 pills - $136.15
- 90 pills - $184.46
- 120 pills - $232.78
- 180 pills - $329.40
- 270 pills - $474.34
Fosamax dosages: 70 mg, 35 mg
Fosamax packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills
In stock: 629
Only $0.49 per item
Description
The most common organisms responsible for wound infections in order of frequency are Staphylococcus species menopause 041 generic fosamax 70 mg with amex, coagulase-negative Streptococcus, enterococci, and Escherichia coli. Most surgical wound infections become apparent within 7 to 10 days postoperatively, although a small number manifest years after the original operative intervention. With the hospital stay becoming shorter and shorter, many infections are detected in the outpatient setting, leading to underreporting of the true incidence of wound infections absent intensive surveillance. The narrowest definition would include wounds that drain purulent material with bacteria identified on culture. The more broad definition would include all wounds draining pus, whether or not the bacteriologic studies are positive; wounds that are opened by the surgeon; and wounds that the surgeon considers infected. About three fourths of all wound infections are superficial, involving skin and subcutaneous tissue only. Clinical diagnosis is easy when a postoperative wound looks edematous and erythematous and is tender. Often the presentation is more subtle, and development of postoperative fever, usually low-grade; development of a mild and unexplained leukocytosis; or the presence of undue incisional pain should direct attention to the wound. Inspection of the wound is most useful in detecting subtle edema around the suture or staple line, manifested as a waxy appearance of the skin, which characterizes the early phase of infection. If a wound infection is suspected, several stitches or staples around the most suspicious area should be removed with insertion of a cottontipped applicator into the subcutaneous area to open a small segment of the incision. Presence of pus mandates further opening of the subcutaneous and skin layers to the full extent of the infected pocket. Samples should be taken for aerobic and anaerobic cultures, with very few patients requiring antibiotic therapy. Patients who are immunosuppressed (diabetics and those on steroids or chemotherapeutic agents), who have evidence of tissue penetration or systemic toxicity, or who have had prosthetic devices inserted (vascular grafts, heart valves, artificial joints, or mesh) should be treated with systemic antibiotics. The incision may drain pus spontaneously, or the intra-abdominal extension may be recognized following the drainage of what was thought to be a superficial wound infection, but pus draining between the fascial sutures will be noted. This is an invasive process that involves the fascia and leads to secondary skin necrosis. Pathophysiologically, it is a septic thrombosis of the vessels between the skin and the deep layers. The skin demonstrates hemorrhagic bullae and subsequent frank necrosis, with surrounding areas of inflammation and edema. The fascial necrosis is usually wider than the skin involvement or than the surgeon estimates on clinical grounds. The patient is toxic and has high fever, tachycardia, and marked hypovolemia, which if uncorrected, progresses to cardiovascular collapse. Bacteriologically, this is a mixed infection, and samples should be obtained for Gram stain smears and cultures to aid in diagnosis and treatment. As soon as bacteriologic studies have been obtained, highdose penicillin treatment needs to be started (2040 million U/d intravenously) due to concern over the presence of Clostridia perfringens and other related species; broad-spectrum antibiotics should be added and the regimen modified based on culture results.
Fraxinus excelsior (Ash). Fosamax.
- What is Ash?
- Dosing considerations for Ash.
- How does Ash work?
- Fever, arthritis, gout, bladder complaints, constipation, increasing urine production (diuretic), and other conditions.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96308
The disease is self-limited in the majority of patients list of women's health issues 70 mg fosamax buy free shipping, and treatment is not required in these cases. Therapy should be considered for (a) patients with impaired cellular immunity; (b) comorbid illnesses that are adversely impacted by the infection, including chronic pulmonary dysfunction, renal failure, and congestive heart failure; and (c) when symptoms and radiographic findings persist for more than 6 to 8 weeks, at which time the disease is considered to be persistent coccidioidal pneumonia and occurs in approximately 1% of patients. Progression to caseous nodules, cavities, and calcified, fibrotic, or ossified lesions indicates complicated or residual stages of coccidioidomycosis. There are several relative indications for surgery in pulmonary coccidioidomycosis. A rapidly expanding (>4 cm) cavity that is close to the visceral pleura is a high risk for rupture into the pleural space and subsequent empyema. Other indications for operative intervention include life-threatening hemoptysis; hemoptysis that is persistent despite medical therapy; symptomatic fungus ball; bronchopleural fistula; cavitary lesions with persistent positive sputum; and pulmonary nodules that degenerate over time. Finally, any nodule with signs that are concerning for malignancy should undergo further evaluation, including biopsy or resection, to determine the underlying etiology. Diagnosis of coccidioidomycosis is confirmed by histopathologic, mycologic, and serologic evaluation. Immunocompromised patients are especially susceptible to disseminated coccidioidomycosis, which carries a mortality rate over 40%. Treatment options for this disease vary depending on the severity of the disease as well as the stage. Amphotericin B deoxycholate or the triazoles continue to be the primary antifungal medications. Blastomyces dermatitidis is a round, single-budding yeast with a characteristic thick, refractile cell wall. Exposure occurs when contaminated soil is disturbed and the conidia are aerosolized. A small minority of patients will develop chronic pulmonary infection or disseminated disease, including cutaneous, osteoarticular, and genitourinary involvement. Symptoms are nonspecific and consistent with chronic pneumonia in 60% to 90% of patients. They include cough, mucoid sputum production, chest pain, fever, malaise, weight loss, and, uncommonly, hemoptysis. In acute disease, radiographs are either completely negative or have nonspecific findings; in chronic disease, fibronodular lesions (with or without cavitation) similar to tuberculosis are noted. Mass lesions similar to carcinoma are frequent, and lung biopsy is frequently used. Over 50% of patients with chronic blastomycosis also have extrapulmonary manifestations, but less than 10% of patients present with severe clinical manifestation. In the absence of therapy, close follow-up is warranted for evidence of progression to chronic or extrapulmonary disease. After adequate drug therapy, surgical resection of known cavitary lesions should be considered because viable organisms are known to persist in such lesions. Most clinicians would agree that losing over a liter of blood via the airway within 1 day is significant, yet use of an absolute volume criterion presents difficulties.
Specifications/Details
Rarely women's health center groton ct cheap fosamax 35 mg on line, if ever, can an aggressive surgical infection be cured only by the administration of antibiotics, and never in the face of an ongoing source of contamination. Also, it has been repeatedly demonstrated that delay in operative intervention, whether due 142 to misdiagnosis or the need for additional diagnostic studies, is associated with increased morbidity and occasional mortality. Prophylaxis consists of the administration of an antimicrobial agent or agents prior to initiation of certain specific types of surgical procedures in order to reduce the number of microbes that enter the tissue or body cavity. Agents are selected according to their activity against microbes likely to be present at 3 the surgical site, based on knowledge of host microflora. For example, patients undergoing elective colorectal surgery should receive antimicrobial prophylaxis directed against skin flora, gram negative aerobes, and anaerobic bacteria. There are a wide variety of agents that meet these criteria with recently published guidelines. However, patients who undergo complex, prolonged procedures in which the duration of the operation exceeds the serum drug half-life should receive an additional dose or doses of the antimicrobial agent. Empiric therapy comprises the use of an antimicrobial agent or agents when the risk of a surgical infection is high, based on the underlying disease process. Obviously, prophylaxis merges into empirical therapy in situations in which the risk of infection increases markedly because of intraoperative findings. Empirical therapy also often is employed in critically ill patients in whom a potential site of infection has been identified and severe sepsis or septic shock occurs. Invariably, empirical therapy should be limited to a short course of drug (3 to 5 days), and should be curtailed as soon as possible based on microbiologic data. Similarly, empirical therapy merges into therapy of established infection in some patients as well. However, among surgical patients, the manner in which therapy is employed, particularly in relation to the use of microbiologic data (culture and antibiotic sensitivity patterns), differs depending on whether the infection is monomicrobial or polymicrobial. Evidence of systemic inflammatory response syndrome (fever, tachycardia, tachypnea, or elevated leukocyte count) in such individuals, coupled with evidence of local infection. An appropriate approach to antimicrobial treatment involves de-escalation therapy, where initial antimicrobial selection is broad, with a later narrowing of agents based on patient response and culture results. Appropriate Use of Antimicrobial Agents Gram-negative microbes, yeast), coupled with institutional and unit-specific drug sensitivity patterns. It is important to ensure that antimicrobial coverage chosen is adequate, since delay in appropriate antibiotic treatment has been shown to be associated with significant increases in mortality. A critical component of this approach is appropriate collection of culture specimens to allow for thorough analysis, since within 48 to 72 hours, culture and sensitivity reports will allow refinement of the antibiotic regimen to select the most efficacious agent. Although the primary therapeutic modality to treat polymicrobial surgical infections is source control as delineated previously, antimicrobial agents play an important role as well. Culture results are of lesser importance in managing these types of infections, as it has been repeatedly demonstrated that only a limited cadre of microbes predominate in the established infection, selected from a large number present at the time of initial contamination.
Syndromes
- Agitation
- Does it cause pain?
- Too much fluoride from environmental sources (natural high water fluoride levels) or overuse of fluoride rinses, toothpaste, and fluoride supplements
- When you are running errands, try parking at the far end of the parking lot, or even down the street. Even better, walk to the store.
- Doppler/ultrasound of the heart (echocardiogram)
- Appears weak
- Kidney failure
- Bone sores (lesions)
- Macroglobulinemia of Waldenstrom
Related Products
Additional information:
Usage: b.i.d.
Tags: order fosamax 35 mg visa, 70 mg fosamax order, fosamax 35 mg purchase mastercard, generic fosamax 35 mg on-line
9 of 10
Votes: 33 votes
Total customer reviews: 33
Customer Reviews
Tarok, 40 years: Due to associated parenchymal injury, subdural hematomas have a much worse prognosis than epidural collections.
Ismael, 33 years: Involvement of a speech and swallowing therapist is critical in the preoperative counseling and postoperative rehabilitation of patients with laryngeal cancer.
Deckard, 42 years: Mycophenolate is the prodrug of mycophenolate acid, derived from Penicillium fungi.
Daryl, 32 years: Typically, a Nikolsky sign develops in which lateral pressure causes the epidermis to detach from the basal layer.
Kasim, 44 years: This avoids thermal injury outside of the operative field and also prevents exit of current through electrocardiographic leads, other monitoring devices, or permanent pacemakers or defibrillators.