- info@careermakers.edu.np
- +977 1 4423870
Sumycin
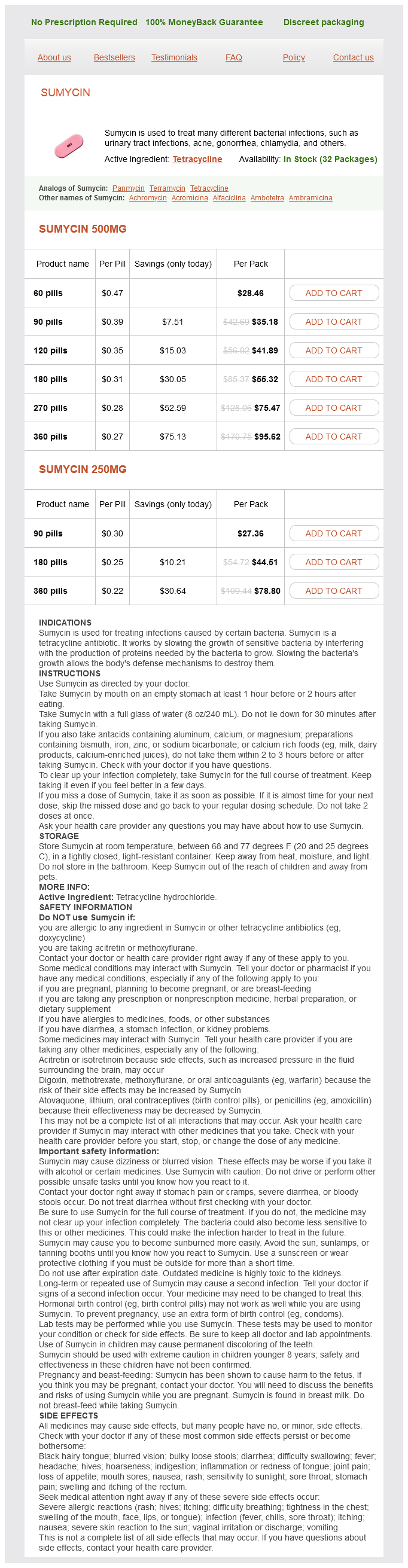
Sumycin 500mg
- 60 pills - $28.46
- 90 pills - $35.18
- 120 pills - $41.89
- 180 pills - $55.32
- 270 pills - $75.47
- 360 pills - $95.62
Sumycin 250mg
- 90 pills - $27.36
- 180 pills - $44.51
- 360 pills - $78.80
Sumycin dosages: 500 mg, 250 mg
Sumycin packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 858
Only $0.23 per item
Description
Riluzole is generally well tolerated by patients; nausea bacteria and archaea are similar in which of the following sumycin 500 mg with amex, gastrointestinal upset, and raised transaminase enzyme levels may occur but are often transient and self-limiting. Clinical trials of many different agents including branched-chain amino acids, dextromethorphan, total lymphoid irradiation, the free radical scavenger acetylcysteine, gabapentin, creatine, vitamin E, lithium, coenzyme Q10, olesoxime, pentoxyfilline, glatiramer acetate, dexpramipexole have all proven negative to date. There was no effect on survival and the medication is not currently licensed for use in Europe. Symptomatic therapy In contrast to the limited disease-modifying therapeutic options, much can be done to address symptoms, disability, and distress. A multidisciplinary setting appears to improve survival in observational studies and usually includes a neurologist, specialist nurse, respiratory, anaesthetic and gastroenterology expertise (for noninvasive ventilation and gastrostomy insertion), speech and language therapist, physiotherapist, occupational therapist, social worker, and links to palliative care medicine. Charities, such as the Motor Neuron Disease Association in the United Kingdom, are often able to facilitate equipment provision. Respiratory function can be monitored clinically, and through forced/slow vital capacity, noninvasive random capnography and capillary blood gases, and augmented by overnight oximetry and capnometry when necessary. Cough assist devices are used to help clear respiratory secretions, and have hypothetical advantages in preventing aspiration pneumonia; a clinical trial is required to assess whether there is any survival benefit. Many patients prefer, and many clinicians advise, to avoid endotracheal intubation in a disease causing such widespread and irreversible weakness, as a locked-in syndrome is the end result. Excess salivation can be a significant problem, especially for patients with bulbar disease, and can be effectively treated using anticholinergics, such as hyoscine patches, sublingual atropine drops, glycopyrronium, amitriptyline tablets, or botulinum toxin injection to the salivary glands. Early swallowing problems may be addressed by simple measures such as a chin tuck, attention to food consistency, and nutritional supplements. Later, more severe dysphagia can be treated with a gastrostomy tube inserted either under endoscopic or radiological guidance. Some centres now perform a hybrid technique, which allows a larger diameter, more secure tube to be placed without conscious sedation, and in the presence of noninvasive ventilation, an important consideration as gastrostomy insertion becomes more risky with respiratory weakness, especially when forced vital capacity falls below 50%. Patients and clinicians may consider gastrostomy in the presence of significant weight loss, recurrent aspiration pneumonia, or when frequent choking or dysphagia makes mealtimes prolonged or intolerable. The aims are to avoid a hungry, dysphagic patient unable to fulfil their nutritional requirements and to facilitate discharge home. Multifocal motor neuropathy with conduction block Patients may present at any stage of adult life with multifocal and slowly progressive muscle weakness over as much as 20 years. The condition is neurophysiologically heterogeneous, ranging from isolated muscle denervation changes on electromyography through classical multifocal conduction block in motor nerves on nerve conduction studies, and occasionally a diffuse demyelinating, pure, motor peripheral neuropathy. There may be no electrophysiological abnormality in early cases or if conduction block is proximal. Spontaneous remissions occur only occasionally, and usually in the subacute subgroup. High-dose intravenous human immunoglobulin (IvIg) therapy can produce dramatic improvement lasting 68 weeks and repeat administration is the mainstay of treatment in symptomatic patients. With IvIg administered sufficiently regularly to prevent end-of-dose deterioration, progressive motor axonal loss can be largely or completely prevented. Steroid therapy does not improve multifocal motor neuropathy, and may precipitate further deterioration.
Hippocastani Cortex (Horse Chestnut). Sumycin.
- What is Horse Chestnut?
- Varicose veins and other circulatory problems (chronic venous insufficiency).
- Are there safety concerns?
- Pain, tiredness, tension, swelling in the legs, itching, and water retention (edema).
- How does Horse Chestnut work?
- What other names is Horse Chestnut known by?
- Are there any interactions with medications?
- Dosing considerations for Horse Chestnut.
- Hemorrhoids, diarrhea, fever, cough, enlarged prostate, eczema, menstrual pain, soft tissue swelling from bone fracture and sprains, arthritis, rheumatism, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97006
If there is no clearly defined aetiology antibiotics for sinus infection dosage cheap sumycin 250 mg free shipping, the dystonia can be classified as idiopathic familial or idiopathic sporadic. Younger age at onset, particularly during childhood, is more likely to be of genetic aetiology and likely to spread to involve a greater number of body parts. The known genetic forms include all monogenic inheritance patterns (autosomal recessive, autosomal dominant, and X-linked). Mutation-carrying subjects exhibit abnormalities of brain metabolism as assessed by fluorodeoxyglucose positron emission tomography analysis, regardless of clinical status Autosomal dominant inheritance with low phenotypic penetrance (around 30% to 40%) indicates other important environmental and/ or genetic factors that affect expression. In fact, an affected patient may have asymptomatic or paucisymptomatic relatives who carry the familial mutation. Mutation carriers who do not develop dystonia by their early 20s almost always remain symptom-free for life, suggesting the presence of a developmental window of susceptibility during which torsin A function is critical for brain function. The disease typically begins in school-aged children, with a mean age at onset of c. Two clinical findings are observed with reasonable consistency: (1) the onset of symptoms before the age of 20 years and (2) the onset of symptoms in the limbs, mainly the legs. The dystonia in most cases was slowly progressive segmental with craniocervical and upper-limb involvement with rare generalization. Clinically, focal dystonia (predominantly cervical dystonia) with minor facial involvement, upperlimb involvement, and spasmodic dysphonia are observed without generalization. The range of age at onset of a slowly progressive predominantly cervical dystonia varies from early childhood to the forties. Laryngeal dystonia and arm involvement is known, whereas the legs are never affected. Penetrance is low (approximately 30%), but may be up to 100% if atypical presentations are considered. Over 90% patients present initially with focal dystonia of the limbs, cranial dystonia, and oromandibular dystonia is less common. The dystonia is progressive for few years and mostly becomes generalized by two years There is a gradual tendency for the dystonia to revert as the disease evolves between the fifth and seventh years after onset. The dystonia is gradually replaced by bradykinesia until an overall presentation of rigidity is reached. Onset is in adolescence or early adulthood with sudden onset of dystonia and parkinsonism, which can develop within minutes or days of onset and are frequently triggered by a psychological stressor. The dystonia and parkinsonism have a clear rostrocaudal gradient: the bulbar symptoms are more severe than the symptoms in the upper limbs, which in turn are more severe than the symptoms in the lower limbs. Initially predominantly focal limb dystonia causing gait and writing problems is followed by generailzed dystonia occurring between two and eitgteen years of age. Most of the patients have pyramidal signs and dopa unresponsive parkinsonism is described in some patients.
Specifications/Details
Acute behavioural disturbance antimicrobial wound cream for dogs 250 mg sumycin buy otc, such as agitation or aggression may be treated with a combination of haloperidol (5 mg) and lorazepam (2 mg). The subsequent regular drug treatment should usually be with a low-potency first generation antipsychotic drug such as chlorpromazine (at a dose of 400600 mg daily), or a secondgeneration antipsychotic drug such as risperidone (46 mg daily) or olanzapine (1015 mg daily). With the reduction in the numbers of psychiatric beds, there is an emphasis on treatment outside of hospital. Predictors of outcome Acute onset and good premorbid functioning predict a better prognosis. Living in a developing country may be associated with a better overall outcome, possibly because of greater social support. Medical morbidity Most people with schizophrenia die of heart attacks, cancer, and strokes, and they do so approximately 1015 years earlier than population average. This shortened life expectancy is attributable to both behaviour and circumstance; most patients smoke heavily and many drink to excess. There is a major medical challenge in correcting the current underinvestigation and undertreatment of these serious medical conditions in people with schizophrenia. Maintenance treatment Numerous randomized trials have found that maintenance use of antipsychotic medication reduces relapse rates at over one year compared to placebo (drugs 27% vs. A smaller dose of antipsychotic drug is often sufficient for maintenance and may enhance compliance. Esterified preparations of antipsychotic drugs allow them to be given as slow releasing fat-soluble depot injections every two to four weeks for patients who want that (rather than taking pills every day), or for those who need to be treated against their will. Approximately one-third of patients will not adequately respond to first- or second-line treatments. Various psychological and social interventions including cognitive behavioural treatment, illness education, and family intervention can reduce the relapse rate. Members of the multidisciplinary community mental health teams can provide these and other services. Antipsychotic drugs versus placebo for relapse prevention in schizophrenia: a systematic review and meta-analysis. Psychological interventions for psychosis: a meta-analysis of comparative outcome studies. Towards the identification of imaging biomarkers in schizophrenia, using multivariate pattern classification at a single-subject level. Somatic symptom disorder of mild severity is common in medical clinics; it usually responds to simple explanation and reassurance. More severe somatic symptom disorder with multiple symptoms and severe disability is less common, but important to diagnose because these patients are at substantial risk of iatrogenic harm from excessive investigation and speculative medical or surgical treatment. Severe somatic symptom disorder usually requires multidisciplinary care, including liaison psychiatry.
Syndromes
- You have had a kidney transplant and your doctor wants to check how well it is working and to look for signs of rejection
- Meningitis - staphylococcal
- Activated charcoal
- Increased body hair (hirsutism)
- Do you have any other symptoms like dry mouth or joint discomfort?
- Swelling (edema)
Related Products
Additional information:
Usage: q.3h.
Tags: buy 250 mg sumycin mastercard, sumycin 250 mg buy low price, sumycin 500 mg purchase with amex, sumycin 250 mg buy free shipping
9 of 10
Votes: 177 votes
Total customer reviews: 177
Customer Reviews
Hogar, 24 years: Aside from supportive care, treatment is with immunosuppression, often comprising corticosteroids with intravenous immunoglobulin and/or plasma exchange. The saphenous nerve is sometimes damaged in surgery for the treatment of varicose veins.
Gancka, 45 years: Sequencing techniques are not always best placed to detect specific types of mutations and partial or whole gene deletions/duplications require a different approach. Good Practice in Service User Involvement in Maternity: Involving Women to Improve their Care.
Abe, 34 years: A clinical response is seen in 90% of patients by the second week of treatment (Table 24. Type I or classic lissencephaly this is the most common type and is characterized by a smooth or almost smooth cerebral surface.
Tangach, 41 years: The usual mistake is to regard as trigeminal neuralgia pain that which is due to some other cause. Development of hypertension will require investigation for phaeochromocytoma, and spinal deformity may need orthopaedic attention.
Bradley, 64 years: The anaesthesia extends upwards on the posterolateral aspect of the calf in its lower two-thirds. Broad-spectrum antibiotics target a wide range of bacteria whereas narrow-spectrum ones target specific types.