- info@careermakers.edu.np
- +977 1 4423870
Antabuse
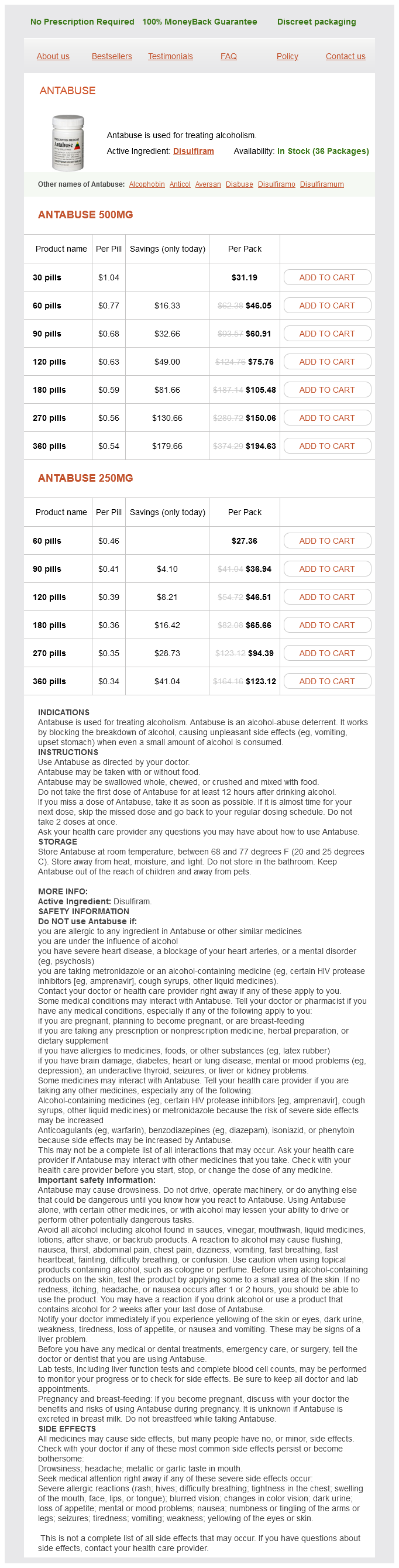
Antabuse 500mg
- 30 pills - $31.19
- 60 pills - $46.05
- 90 pills - $60.91
- 120 pills - $75.76
- 180 pills - $105.48
- 270 pills - $150.06
- 360 pills - $194.63
Antabuse 250mg
- 60 pills - $27.36
- 90 pills - $36.94
- 120 pills - $46.51
- 180 pills - $65.66
- 270 pills - $94.39
- 360 pills - $123.12
Antabuse dosages: 500 mg, 250 mg
Antabuse packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 809
Only $0.36 per item
Description
This is particularly important in infants and children where an assistant may be called upon to hold the patient in position medications used to treat ptsd generic 500 mg antabuse mastercard. Identify by palpation the vertebral spinous processes in the midline and the posterior superior iliac spines. The patient can help to determine if the needle is in the midline by providing real-time feedback of where they feel the needle. Another option is to draw a line between the spinous process of C7 and the gluteal cleft. Adjust the bed height so that you can sit in a comfortable position while performing the procedure. Place povidone iodine or chlorhexidine solution into the basin provided with the kit. Apply povidone iodine or chlorhexidine solution using a circular motion from the intended site of entry outward. Midsagittal section of the lumbosacral region with a spinal needle in the L3-L4 interspace. The needle has penetrated the supraspinal ligament, the interspinous ligament, the ligamentum flavum, the dura mater, and the arachnoid mater. Place a skin wheal of local anesthetic solution subcutaneously over the desired interspace using a 25 gauge needle. Infiltrate and anesthetize the deeper tissue of the interspace along the projected needle track using the 22 gauge needle. The infiltration of local anesthetic solution, unless contraindicated, should be used in all patients, including neonates and young children. The interspinous ligament and the periosteum are supplied by the recurrent spinal nerves branching off the nerve roots exiting the spinal canal at the same level. The topical anesthetic only anesthetizes the skin and superficial subcutaneous structures. It may occasionally be difficult for some patients to remain still and cooperative with the procedure. This can include anxious patients, those with an altered mental status, and small children. These patients may require an intravenous anxiolytic, nitrous oxide administration (Chapter 158), or procedural sedation (Chapter 159). Orient the bevel of the spinal needle parallel to the longitudinal dural fibers to increase the chances that the fibers will be separated rather than cut by the tip of the needle. Resistance will usually be felt as the needle penetrates the interspinous ligaments. If bone is still encountered, redirect the needle slightly more cephalad and readvance it. Attach the stopcock and manometer directly to the needle or use the short extension tubing provided in most kits as a spacer.
Witch Meal (Club Moss). Antabuse.
- Are there safety concerns?
- Bladder and kidney disorders.
- What is Club Moss?
- How does Club Moss work?
- Dosing considerations for Club Moss.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96068
Patients presenting with cranial nerve injuries associated with the dislocation require emergent consultation prior to the reduction symptoms zenkers diverticulum 500 mg antabuse buy mastercard. Note the mandibular condyle is anterior to the articular eminence of the temporal bone. Place the patient sitting in a multipositional procedure chair with a solid headrest to support their head. Adequate analgesia and muscle relaxation will allow easier manipulation of the mandible back into its anatomic position. Strongly consider the use of parenteral analgesics, sedatives, and/or muscle relaxants. This is especially true to relax the muscles of mastication and allow reduction if the mandible has been dislocated for more than 6 to 8 hours. Sagittal computed tomography scan image demonstrating the mandibular condyle (arrow) is dislocated anteriorly to the articular eminence (arrowhead). The risk of a bite injury to the Emergency Physician is real and might lead to a transmittable disease. This technique often requires procedural sedation to overcome the muscles of mastication. These are too small to make a recommendation and are not endorsed by the author of this chapter and book editor. The gauze squares on the thumbs are to prevent possible lacerations to the Emergency Physicians thumbs when the mandible reduces. Alternatively, place the thumbs on the mandibular ridge immediately posterior to the molars. The downward pressure releases the mandibular condyle from the articular eminence of the temporal bone while manipulating the condylar head and seating it back in the articular glenoid fossa. Instruct the patient to open their mouth further to relax the elevators of the mandible and to accentuate the deformity. Instruct the patient to gently bite the syringe while rolling it back and forth in their mouth. Proper thumb and hand placement for the reduction of an anteriorly dislocated mandible. Apply downward pressure with the thumbs (1) followed by posteriorly directed pressure (2) to reduce the dislocation. Apply upward pressure with the thumbs while simultaneously applying downward pressure on the mandible with the fingers to unlock the mandible and reduce the dislocation. Place a thumb above the dislocated coronoid process and the fingers of that hand behind the mastoid process. Place the other thumb over the malar eminence with the fingers of that hand over the angle of the mandible.
Specifications/Details
The goal is to deliver the fetus as quickly as possible using safe maneuvers and documenting the chain of events symptoms joint pain effective antabuse 500 mg. The incidence of shoulder dystocia varies due to the subjective nature of the diagnosis and the dependency on the documentation. It results from impingement of the biacromial diameter of the fetus against the maternal pubic symphysis anteriorly and the maternal sacral promontory posteriorly. The Emergency Physician must deliver the fetus quickly and without applying excessive forces that may result in fetal injury. Associated risk factors include fetal macrosomia, maternal diabetes, multiparity, obesity, operative vaginal delivery, prior history of shoulder dystocia or macrosomia, prolonged second stage of labor, and postterm pregnancy (Table 164-1). More aggressive approaches may be indicated in cases that are refractory to successful delivery of the neonate. Reevaluate the course of action including using other maneuvers or repeating maneuvers. A symphysiotomy (Chapter 168) is indicated for shoulder dystocia unresponsive to less invasive techniques and for fetal head entrapment by presumed cephalopelvic disproportion. The Emergency Physician is usually only managing precipitous deliveries where there is no other personnel trained in the management of laboring patients. The indications to perform a cesarean delivery are relative contraindications for release maneuvers. Resist applying excessive downward or lateral traction on the fetal head and neck. Avoid applying fundal pressure and discontinue maternal pushing efforts until disimpaction has occurred. Fundal pressure and maternal pushing may further impact the fetal shoulders, increase the risk of uterine rupture, and should never be performed. Notify the medical personal in the room of the situation and summon extra personnel for help with one person designated as a timekeeper. Notify a Neonatologist of the impending delivery and contact an Anesthesiologist for pain control. Include fetal distress, fetal death, fetal hypoxia, and hysterectomy in the discussion. There is often not enough time to obtain a written consent in the Emergency Department. Pain associated with the first stage of labor can be relieved with a paracervical block or pudendal nerve block.
Syndromes
- Weakness
- Do not run a humidifier for a long time. If room surfaces are constantly damp or wet to the touch, mold and mildew can grow. This can cause breathing problems in some people.
- Breathing
- Keep your child informed of necessary and anticipated changes such as changes in jobs or moving
- Coffee or tea
- Medicines (for example, certain diet drugs)
- Lack of protein, vitamins, minerals, and other important nutrients in the body (malnutrition)
- Precancerous polyps (nodes)
- Name of product (as well as the ingredients and strength if known)
Related Products
Additional information:
Usage: q._h.
Tags: antabuse 500 mg buy, buy 250 mg antabuse with amex, buy antabuse 250 mg without a prescription, generic antabuse 250 mg online
8 of 10
Votes: 58 votes
Total customer reviews: 58
Customer Reviews
Umul, 62 years: Fat pad atrophy on the plantar aspect of the foot can result in painful ambulation and gait disturbances.
Marlo, 39 years: Avoid hypodermoclysis in the patient with anticoagulation, blood dyscrasias, circulatory failure, fluid overload states.