- info@careermakers.edu.np
- +977 1 4423870
Augmentin
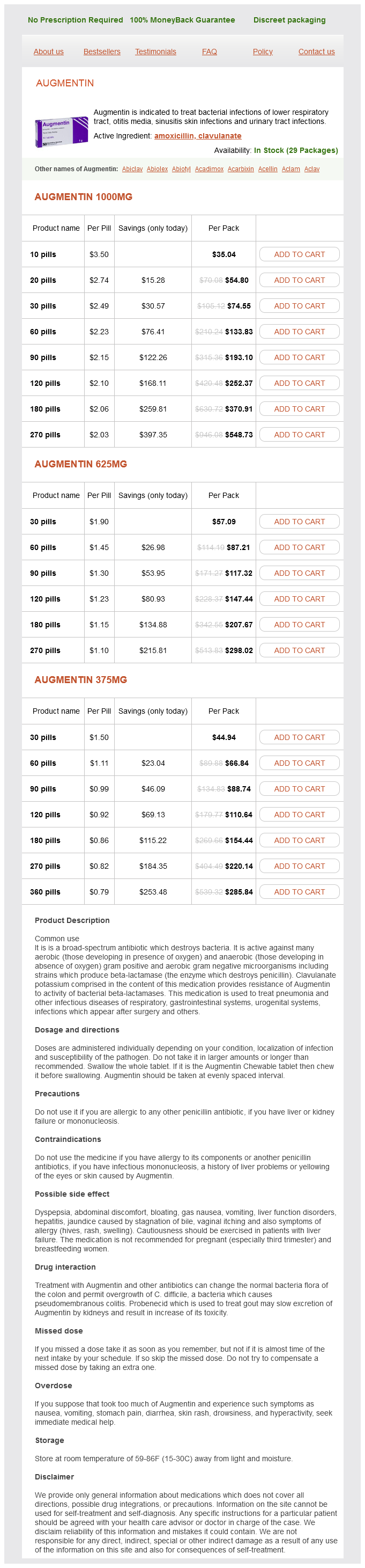
Augmentin 1000mg
- 10 pills - $35.04
- 20 pills - $54.80
- 30 pills - $74.55
- 60 pills - $133.83
- 90 pills - $193.10
- 120 pills - $252.37
- 180 pills - $370.91
- 270 pills - $548.73
Augmentin 625mg
- 30 pills - $57.09
- 60 pills - $87.21
- 90 pills - $117.32
- 120 pills - $147.44
- 180 pills - $207.67
- 270 pills - $298.02
Augmentin 375mg
- 30 pills - $44.94
- 60 pills - $66.84
- 90 pills - $88.74
- 120 pills - $110.64
- 180 pills - $154.44
- 270 pills - $220.14
- 360 pills - $285.84
Augmentin dosages: 1000 mg, 625 mg, 375 mg
Augmentin packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 779
Only $0.84 per item
Description
Rarely antibiotic resistance peter j collignon purchase augmentin 1000 mg otc, the granulomatous gastritis is idiopathic (diagnosis made after exclusion of all known causes). These patients are usually older than 40 years, and present with epigastric pain, weight loss and vomiting secondary to pyloric obstruction. Gastritis in immunosuppressed patients these patients are prone to infection by various viruses including cytomegalovirus, herpes simplex and bacteria (Mycobacterium avium-intracellulare) and parasites. In infections by cytomegalovirus, the histology shows the typical intranuclear eosinophilic inclusions with a patchy mild inflammatory infiltrate. Infections with herpes simplex are diagnosed by basophilic intranuclear inclusions in epithelial cells. Gastric mucosal biopsy confirms necrosis and intracellular trophozoites in gastric epithelial, smooth muscle and endothelial cells. Eosinophilic gastritis this occurs as part of eosinophilic gastroenteropathy in children and adults below 50 years and has an allergic basis (allergy to milk or soya protein especially in children). Eosinophilic gastroenteritis can also be found in patients with connective tissue disorders (polyarteritis nodosa, scleroderma, polymyositis and dermatomyositis). Radiation gastritis Although small doses of radiation (up to 1500 R) cause reversible mucosal damage, higher radiation doses induce irreversible damage with atrophy and ischaemic-related ulceration from submucosal endarteritis. The severely damaged mucosa causes repeated episodes of bleeding and may require resection. Gastric tumours 601 Suppurative (phlegmonous) gastritis this is a rare and often fatal bacterial infection producing a cellulitis of the stomach wall. The condition usually complicates a pre-existing gastric lesion and is more commonly encountered in elderly and alcoholic patients. At operation, the stomach exhibits a dusky discoloration and its serosal surface is covered with a fibrinous exudate. Necrotizing gastritis is an especially severe variant which results in overt infective gangrene. It is caused by a mixed infection with fusiform and spirochaete bacteria from the mouth. Emphysematous gastropathy Air-filled cysts in the gastric wall are rare and usually accompanied by pneumatosis cystoides intestinalis. Gas cysts in the wall of the stomach can also occur in association with pyloric obstruction and chronic obstructive airway disease with emphysema. Gas can also be introduced in the wall of the stomach following incomplete injuries during endoscopy. In support of this observation, the gastric cancer incidence in migrants from low-incidence countries increased from a low rate in first-generation migrants to high incidence of their host country in the second generation. Even assuming the current decline, the incidence of gastric cancer will continue: the predicted growth in the world population combined with the increased longevity will most likely result in a net increase in the overall number of gastric cancers being diagnosed.
Paradisapfel (Grapefruit). Augmentin.
- How does Grapefruit work?
- Are there any interactions with medications?
- Are there safety concerns?
- Asthma, lowering cholesterol, hardening of the arteries (atherosclerosis), preventing cancer, weight loss, psoriasis, muscle fatigue, promoting hair growth, toning the skin, reducing acne and oily skin, treating headaches, stress, depression, infections, digestive complaints in people with eczema, yeast infections (as a vaginal douche), and other conditions.
- Dosing considerations for Grapefruit.
- What is Grapefruit?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96909
Recognized postintubation pulmonary complications can be divided into long term and short term antimicrobial resistance in developing countries buy 1000 mg augmentin with visa. It is, however, difficult to prove causality arising from the surgical procedure itself, as many patients undergoing this type of surgery will have pre-existing pulmonary pathologies. Not surprisingly, duration of the operation seems to be as important as the time of postoperative mechanical ventilation. These include regular mouthwashes for oral decontamination, establishing early enteral feeding and stress ulcer prophylaxis. Ventilation with low airway pressures is presumed to limit overdistension of the more rigid alveoli while minimizing harm to non-affected lung parenchyma. Death and organ transplantation the diagnosis, confirmation and certification of death are core medical skills. This might sound obvious and straightforward, but in times when resuscitation techniques are more successful than ever and the medical benefits of organ transplantation are becoming widely recognized, special challenges for the clinician can arise. Owing to mechanical ventilation, respiratory death can be prevented and has transformed the course of many terminal neurological disorders. This has led to the understanding that, along with the definition of cardiorespiratory death, a new Acute lung injury/acute respiratory distress syndrome Severe pulmonary failure is defined by diffusion hypoxia due to a global decreased diffusion capacity of the alveolar membrane. Whereas in cardiorespiratory arrest the cessation of circulation will obviously lead to irreversible loss of brain function, the irreversible loss of brain function with maintenance of circulation has proved a novel concept. To date, medical professionals as well as lay people throughout the world have adopted the concept that a person is dead when his/her brain is dead. This section will outline the principles of the diagnosis of death, with a special emphasis on brain stem testing and the principles of organ donation. Irreversible coma First, the cause for persistent coma needs to be established and any reversibility must be excluded. Potential reversible factors are intoxication by drugs and medication, neuromuscular blocking agents, hypothermia and electrolyte imbalance Table 6. Acute endocrine imbalance associated with brainstem death is not the cause of reversible coma; chronic profound endocrine failures can usually be excluded from the history. Prolonged action and accumulation of hypnotics, tranquilizers and sedatives must be taken into account and sufficient time should be allowed for their clearance. If significant diagnostic uncertainty remains, brainstem testing cannot be undertaken. Death after cardiorespiratory arrest There are currently no standardized criteria in the confirmation of death following irreversible cessation of cardiorespiratory function. As a result, practice still varies worldwide from confirming death as soon as the heart stops or when attempts at cardiopulmonary resuscitation are abandoned to waiting for 10 minutes or longer after the onset of asystole and apnoea. In the primary care setting this practice continues to be appropriate, whereas in hospitals the increasing practice of nonheart-beating organ donation warrants a standardized approach to confirming death. Asystole can be identified by the absence of a central pulse on palpation and absence of heart sounds on auscultation.
Specifications/Details
Metyrapone is useful in controlling the symptoms of cortisol excess in patients who are unfit or unsuitable for surgery antibiotics for steroid acne augmentin 625 mg line. Survival rates for adrenocortical carcinoma are poor and are dependent on disease stage at presentation. Unfortunately most patients at presentation have advanced incurable disease and only palliation is possible. It is caused by excessive aldosterone secretion from the zona glomerulosa of the adrenal cortex. This potentially curable condition accounts for <1% of all patients with hypertension and was first described by Dr Jerome Conn in 1955, 3 years after the hormone aldosterone had been identified. Excessive aldosterone production causes expansion of plasma volume and elevation of the blood pressure (see Physiology). The rise in blood volume and sodium ion concentration is detected by the juxtaglomerular apparatus and renin secretion falls in response. Loss of potassium and hydrogen ions in the urine leads to hypokalaemia and metabolic alkalosis. Other less common causes are bilateral adrenocortical hyperplasia (idiopathic hyperaldosteronism), aldosterone-producing adrenocortical carcinoma, glucocorticoid-suppressible hyperaldosteronism (familial type 1), non-glucocorticoid-suppressible hyperaldosteronism (familial type 2, which may be an adenoma or hyperplasia) and aldosterone-producing ovarian carcinoma. Tumours are composed of lipid-laden clear cells and occur more frequently on the left side. Patients may be symptomless and the diagnosis is often only suspected when routine biochemical analysis characteristically reveals hypokalaemia associated with mild hypernatraemia. Prior to carrying out biochemical studies potassium stores should be replenished (hypokalaemia inhibits aldosterone secretion) and drugs affecting reninaldosterone regulation should be discontinued for 46 weeks. In patients in whom hypertension is marked, antihypertensive medication may be continued with agents such as prazosin and guanethidine, although calcium channel blockers and beta-blockers probably do not significantly affect results. Aldosterone suppression test When results are equivocal further evaluation is deemed necessary. Diagnosis of primary hyperaldosteronism in this situation may be confirmed by failure to demonstrate suppression of urinary aldosterone secretion in response to a sodium load. Caution is necessary in performing these tests as biochemical disturbances can be severe and marked hypokalaemia may ensue. Patients should therefore be normokalaemic prior to testing and have potassium supplementation throughout the test. Oral sodium loading takes place over 3 days at a dose of 9 g/day; on the third day a 24 hour urine collection is made and urinary aldosterone, potassium and sodium levels are measured. The 24 hour urinary sodium excretion should exceed 200 mEq (documenting adequate sodium loading) and the diagnosis of hyperaldosteronism is confirmed if aldosterone levels exceed 12 g. Microscopic and/or macroscopic nodular hyperplasia is a frequently associated feature, present in approximately 4050% of patients. Idiopathic hyperaldosteronism is found in 1015% of patients with primary hyperaldosteronism.
Syndromes
- Human papilloma virus (HPV, or genital warts) infection in women under age 50
- Multiple birth defects
- Vomiting
- Teeth that do not line up properly
- Teach children how to be safe and look out for themselves.
- Underactive thyroid (hypothyroidism)
Related Products
Additional information:
Usage: q.d.
Tags: safe 375 mg augmentin, buy discount augmentin 625 mg on-line, purchase augmentin 625 mg free shipping, generic augmentin 375 mg buy
10 of 10
Votes: 124 votes
Total customer reviews: 124
Customer Reviews
Yussuf, 60 years: This may be a reflection of the primary disease process, or, alternatively, may be a feature of the concomitant use of other drugs. Poor understanding of intrahepatic anatomy in the Western world has also been a contributing factor.
Ballock, 30 years: Fasciotomy is often required when prolonged ischaemia or soft-tissue injury is present. When diarrhoea occurs, amoebae are expelled and can be detected in freshly passed fluid stools.
Kirk, 59 years: The majority of patients are females who classically develop osteomalacia 1020 years after the gastrectomy. Clinical features In the female, the disease causes an acute purulent inflammation of the vulva, cervix, uterus and adnexa.
Rune, 53 years: Most patients in this category have adjusted to the reduced haemoglobin load and the associated haemodilution may be beneficial in ensuring adequate tissue perfusion in the perioperative period. Existence, causes and consequences of hospital and community disease related malnutrition and clinical and financial benefits of nutritional intervention.
Angir, 49 years: Prior to transfer, consider the following problems: hypoxia or airway protection during ·If there is any concern aboutand artificially ventilate the patient. Subsequently a co-ordinated team approach between surgeon and anaesthetist should ensure a safe outcome.
Torn, 28 years: All of the patients in the Stahl study and 90% of the patients in the Bedenne trial had squamous cell carcinoma. Mastectomy is indicated for operable breast cancer which is either large or at multiple sites, when radiotherapy is to be avoided, or by patient preference.
Quadir, 58 years: Glutamine is mobilized preferentially, and serves two unique purposes: it is utilized by gut enterocytes as an energy source and by the kidney for ammonia production. The gallbladder is attached anteriorly some distance to the right of the umbilical fissure.