- info@careermakers.edu.np
- +977 1 4423870
Cozaar
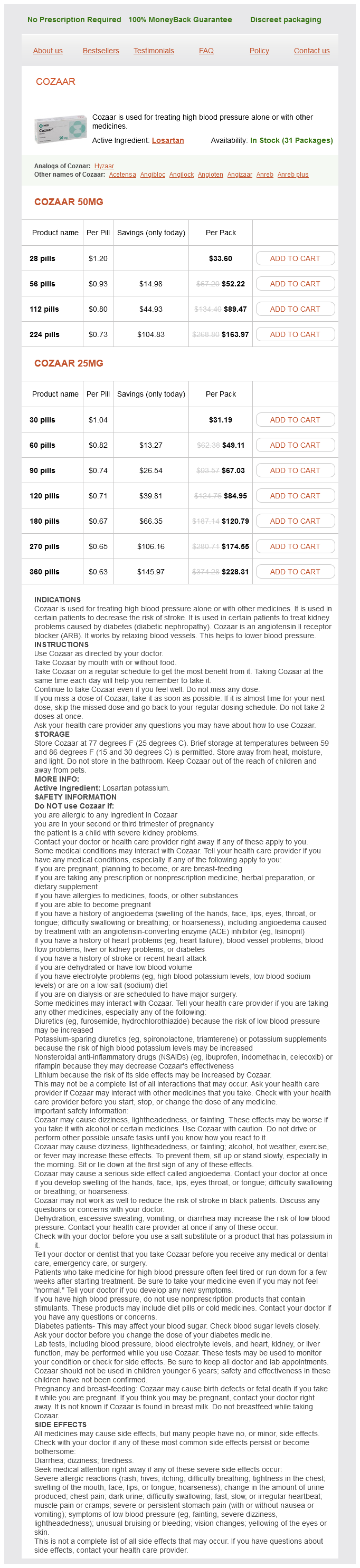
Cozaar 50mg
- 28 pills - $33.60
- 56 pills - $52.22
- 112 pills - $89.47
- 224 pills - $163.97
Cozaar 25mg
- 30 pills - $31.19
- 60 pills - $49.11
- 90 pills - $67.03
- 120 pills - $84.95
- 180 pills - $120.79
- 270 pills - $174.55
- 360 pills - $228.31
Cozaar dosages: 50 mg, 25 mg
Cozaar packs: 28 pills, 56 pills, 112 pills, 224 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 745
Only $0.67 per item
Description
Interleukin-1-induced myocardial depression in an isolated beating heart preparation diabetes symptoms 2013 order cozaar 50 mg amex. Cardiopulmonary dysfunction in a feline septic model: possible role of leukotrienes. Acute adrenal insufficiency presenting as shock after trauma and surgery: three cases and review of the literature. Impaired pressor sensitivity to noradrenaline in septic shock patients with and without impaired adrenal function reserve. A 3-level prognostic classification in septic shock based on cortisol levels and cortisol response to corticotropin. Adrenal insufficiency occurring during septic shock: incidence, outcome, and relationship to peripheral cytokine levels. Stress doses of hydrocortisone reverse byperdynamic septic shock: a prospective randomized, doubleblind, single-center study. Corticosteroid treatment and intensive insulin therapy for septic shock in adults: a randomized controlled trial. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2008. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock, 2012. Does the pulmonary wedge pressure predict left ventricular preload in critically ill patients Importance of venous return, venous resistance, and mean circulatory pressure in the physiology and management of shock. Baroreflex control of regional capacitance and blood flow distribution with or without alpha adrenergic blockade. Selective venoconstriction by dopamine in comparison with isoproterenol and phenylephrine. Determination of total effective vascular compliance in patients with sepsis syndrome. The role of the vasculature in regulating venous return and cardiac output: historical and graphical approach. Applied cardiovascular physiology in the critically ill with special reference to diastole and ventricular interaction. Instantaneous pressure-volume relationships and their ratio in the excised, supported canine left ventricle.
Wuyi Tea (Oolong Tea). Cozaar.
- Mental alertness.
- What other names is Oolong Tea known by?
- Are there safety concerns?
- Are there any interactions with medications?
- Reducing the risk of ovarian cancer.
- Skin allergies, diabetes, high blood pressure, preventing tooth decay, reducing the risk of cancer, osteoporosis, promoting weight loss, and other conditions.
- Dosing considerations for Oolong Tea.
- How does Oolong Tea work?
- What is Oolong Tea?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97045
Crystalloid fluids (such as normal saline solution and lactated Ringer solution) contain sodium chloride in a quantity that closely matches extracellular fluid diabetes test japan cozaar 25 mg purchase online. Colloids, in addition, contain albumin or large osmotically active carbohydrates (hydroxyethylstarch, dextran) that may be held within the intravascular space, resulting in an increase of the plasma oncotic pressure. It has been suggested that in shock associated with microvascular changes of permeability (such as sepsis), colloid fluids remain in the intravascular space, leading to decreased tissue edema and noncardiogenic pulmonary edema. For the most part, meta-analyses have failed to demonstrate clinical outcome superiority of crystalloids compared to either albumin or synthetic colloids. A trend toward improved outcomes with albumin in severe sepsis and saline solution in trauma failed to reach significance in that study. More recently, a substantial body of literature has shown that synthetic colloids increase the risk of renal injury and death, particularly in sepsis and septic shock. Albumin can be considered in septic shock for volume replacement in patients who need substantial amount of crystalloid. Controversy exists on the exact ratio of packed red blood cells, fresh frozen plasma, and platelets. However, more patients achieved hemostasis and fewer died of exsanguination in the 1:1:1 group. The only study to (indirectly) examine blood transfusion in shock suggested that early augmentation of hematocrit to more than 30% during septic shock as part of a protocol to drive cSvO2 to more than 70% was associated with improved survival. Once intravascular volume is optimized, the next line of therapy of circulatory shock usually involves inotropes and vasopressors. Alternately, vasopressors may be occasionally required for brief periods of blood pressure support in extremely hypotensive patients before initiation of fluid infusion. Three major classes of agents are used clinically for inotropic or vasopressor support in critically ill patients: sympathomimetics, phosphodiesterase inhibitors, and vasopressin (antidiuretic hormone) (Table 22. Sympathomimetics (catecholamines) may activate cardiac 1- and -adrenoreceptors, peripheral vascular - or 2receptors, and vascular dopaminergic receptors. Recent uncontrolled studies have shown that endogenous vasopressin concentrations may be relatively deficient in shock states and that infusion of vasopressin (which has little effect in healthy, normotensive subjects), can have a profound pressor effect during vasodilatory shock. It can be used for persistent hypotension despite high-dose dopamine during septic and obstructive shock. It should generally be used only transiently in cardiogenic shock because it may drastically reduce forward flow. Similarly, it should not be required during hemorrhagic shock except for extremely brief periods of blood pressure support pending volume infusion. Infusion rates of 2 to 20 µg/min are commonly used, but if necessary higher rates may be tried. A central and peripheral nervous system neurotransmitter and the biologic precursor of norepinephrine, dopamine stimulates three different receptors; vascular dopaminergic, cardiac 1, and vascular. At infusion rates of less than 4 to 5 µg/kg per minute, dopaminergic effects have been said to dominate, but studies suggest this has little clinical relevance (although in the past it was the theoretical basis for use of low-dose dopamine for renal protection).
Specifications/Details
Although the transition of positive-pressure ventilation is associated with a predictable set of physiologic responses diabetes test in urine cozaar 25 mg buy lowest price, the overall hemodynamic response is largely a consequence of underlying patient comorbid conditions (such as left ventricular dysfunction) and preload status. Immediately after endotracheal intubation, worsening hemodynamics are usually secondary to a decrease in preload, as right atrial pressure will increase, or a drop in arteriolar tone from sedation and analgesia. Any change in hemodynamics in the mechanically ventilated patient should prompt a thorough and almost algorithmic evaluation for potential causes. Shortly after a patient is endotracheally intubated to initiate mechanical ventilation, thoughts should turn toward liberation from the ventilator. The withdrawal of mechanical support is a continuum from intubation until hospital discharge. There are several evidence-based guiding principles that shorten mechanical ventilation days across a broad cohort of critically ill patients. A key component in liberation from the ventilator is the targeted use of sedation, limitation of sedative and opioid infusions, and the monitoring for and aggressive treatment of delirium. This could include sedation, weakness, delirium, respiratory muscle fatigue, or left ventricular dysfunction. Respiratory system compliance is related to the amount of normally aerated lung tissue that remains, the so-called baby lung. This results in the release of biologic inflammatory mediators and the spread of injury to distant organs, causing multiple organ dysfunction syndrome and death. With strong diaphragm contractions during early inspiration spontaneous breathing may lead to regional overinflation and ventilation induced lung injury. This deterioration in oxygenation can occur from infectious and noninfectious conditions. Mechanical ventilation for longer than 48 hours is regarded as the most frequent risk factor. H2-receptor antagonists and proton pump inhibitors have been shown to reduce the incidence of clinically important bleeding compared with sucralfate and are considered the first-line therapy among many clinicians. Pressure is applied in a linear proportion to Edi, and this requires the placement of an esophageal electrode (similar to nasogastric tube placement). A pilot randomized trial comparing weaning from mechanical ventilation on pressure support versus proportional assist ventilation. Developing a new, national approach to surveillance for ventilator-associated events. Standardized rehabilitation and hospital length of stay among patients with acute respiratory failure; a randomized clinical trial.
Syndromes
- Gallstones
- Do you drink alcohol? How much?
- Light-headedness, dizziness
- Time it was swallowed
- Did it develop within 4 to 6 hours after exposure to something that you are or may be allergic to (antigen)?
- Acute unilateral obstructive uropathy
- Has a base that bleeds easily if it is banged or scraped
- Protein C and protein S levels
Related Products
Additional information:
Usage: p.o.
Tags: quality 25 mg cozaar, cheap cozaar 50 mg without a prescription, best 50 mg cozaar, cheap cozaar 50 mg without prescription
9 of 10
Votes: 111 votes
Total customer reviews: 111
Customer Reviews
Joey, 42 years: We must evaluate each patient and use the limited evidence available to us to guide compassionate and rational, if not evidence-based, use of therapy for our patients. Anticoagulation, when required for electrophysiology procedures, such as those involving left atrial ablation, raises the risk substantially.
Mannig, 51 years: Addition of demedetomidine to benzodiazepines for patients with alcohol withdrawal syndrome in the intensive care unit: a randomized controlled study. Airway accidents in intubated intensive care unit patients: an epidemiological study.
Delazar, 30 years: Although some isolated paraspinous infections have been treated with needle aspiration, most will require open surgical incision and drainage along with the administration of systemic antibiotics. Typical hemodynamic profiles of different forms of shock have been described in Table 22.
Gambal, 38 years: Capture thresholds are predictably higher than with endocardial pacing, but most patients will capture at a pacing output of 40 to 70 mA. Although limits customarily regarded as safe are exceeded at the peril of increased risk of serious neurologic morbidity, the treatment protocol that is ultimately applied must, to a degree, be individualized.
Ugo, 60 years: A compliant pericardium can accommodate as much as 1 L of fluid without hemodynamic compromise. Intraoperative cryoneurolysis of intercostal nerves has been reported with good efficacy in controlling postthoracotomy pain (53).
Owen, 41 years: Abolition of protective laryngeal and pharyngeal reflexes may be achieved by inducing a deep level of unconsciousness using one or more of the aforementioned agents, followed by inhalation of high concentrations of a volatile anesthetic agent. Fluid Resuscitation Intravascular volume expansion is another important aspect of sepsis management and is the best initial therapy for the cardiovascular instability of septic shock.