- info@careermakers.edu.np
- +977 1 4423870
Estrace
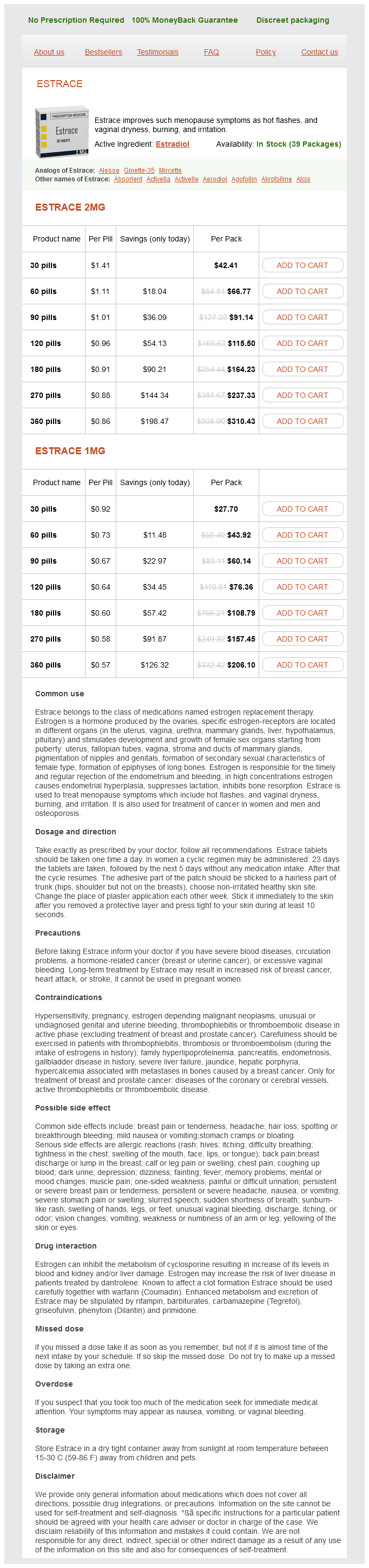
Estrace 2mg
- 30 pills - $42.41
- 60 pills - $66.77
- 90 pills - $91.14
- 120 pills - $115.50
- 180 pills - $164.23
- 270 pills - $237.33
- 360 pills - $310.43
Estrace 1mg
- 30 pills - $27.70
- 60 pills - $43.92
- 90 pills - $60.14
- 120 pills - $76.36
- 180 pills - $108.79
- 270 pills - $157.45
- 360 pills - $206.10
Estrace dosages: 2 mg, 1 mg
Estrace packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 724
Only $0.61 per item
Description
Like the scala vestibuli and scala tympani breast cancer questions for doctor cheap 1 mg estrace visa, the cochlear duct is filled with fluid but the fluid in the cochlear duct is endolymph rather than perilymph (see more later). Importantly, the cochlear duct is flexible, so that pressure waves move the cochlear duct up and down. Because the cochlea is surrounded by unyielding bone, two pressure valves are needed to support any movement of the fluid within. Just as liquid does not come out of a single pinhole in a soda can, movement of the oval window only produces a pressure wave because a second compressible portal, the round window, exists. Compression at the oval window results in rarefaction at the round window, and rarefaction at the oval window produces compression of the round window. Airborne sounds that arrive at different frequencies set up movements of the oval window at corresponding frequencies. The movement of the oval window in turn sets up a pressure wave at a given frequency that travels through the cochlea. Thus, pressure waves at the highest frequency represented in the human cochlea (20,000 Hz) move the cochlear duct at the base of the spiral; pressure waves with low frequencies (less than 200 Hz) move the cochlear duct closest to the helicotrema. An important mechanism of tonotopy is the flexibility of the stiffest part of the cochlear duct, the basilar membrane. Recall that the basilar membrane forms the border between the cochlear duct and the scala tympani. Note that the dimensions of the bony cochlea and those of the cochlear duct are inversely arranged: · the narrowest part of the cochlear duct is located at the widest part of the bony cochlea. The narrow basilar membrane at the base of the cochlea is stiffest and therefore moves maximally in response to high-frequency pressure waves. In contrast, at the apex of the cochlea, the wide basilar membrane is relatively loose and bends maximally in response to low-frequency pressure waves. Consequently, the basilar membrane moves maximally in response to sounds of progressively lower frequencies as one moves from the base of the cochlea to its apex. This topographic arrangement of maximal pressure wave excursion along the length of the cochlea follows a tonotopic organization. The tonotopy of the basilar membrane dictates a tonotopic neural response to sound so that the apical cochlea responds best to low-frequency sounds and the basal cochlea responds best to sounds of high frequency. The frequency that produces the greatest movement of the basilar membrane, and consequently the greatest hair cell response at any one point within the cochlea, is termed the characteristic frequency. Dividing the organ of Corti from the rest of the cochlear duct is the tectorial membrane, which emanates outward from the modiolus, the central pillar of the cochlear spiral. Sensory hair cells sit atop the basilar membrane and extend cellular extensions termed stereocilia into the scala media, the fluid chamber of the organ of Corti. At the outer edge of the cochlear duct is a specialized tissue, the stria vascularis, which pumps potassium ions into the scala media to form endolymph. Endolymph is a potassium ion-rich fluid that fills the scala media, the fluid-filled portion of the cochlear duct. The organ of Corti contains two types of hair cells, inner and outer, and the tectorial membrane (tm).
Chinese Indigo (Isatis). Estrace.
- Are there safety concerns?
- How does Isatis work?
- Prostate cancer, upper respiratory infections, inflammation in the brain, hepatitis, lung abscess, psoriasis, diarrhea, and HIV.
- What is Isatis?
- Dosing considerations for Isatis.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96877
Damage to the cerebellum produces ataxic cerebral palsy breast cancer 49ers cheap estrace 1 mg free shipping, and damage to the basal ganglia produces athetoid cerebral palsy. Maternal infections, placental insufficiency, perinatal trauma, and oxygen deprivation are all potential causes of cerebral palsy. Regardless of the etiology, cerebral palsy results when damage to a motor control or modulatory region occurs. Many, possibly most, spastic cerebral palsy cases result from lesions of the white matter surrounding the ventricles, where axons of the corticospinal tract pass. The pathophysiology of cerebral palsy revolves around competition within the spinal cord between corticospinal axons from the left and right hemispheres. In a healthy baby, corticospinal axons from each motor cortex reach both sides of the spinal cord. With time, contralateral axons dominate ipsilateral axons, and the former make permanent synapses. The ipsilateral axons, on the losing end of this competition, retract their axons. Unfortunately, damage to the corticospinal tract on one side prevents the normal competition between descending axons from the two hemispheres. As a result, ipsilateral corticospinal axons do not retreat from the spinal cord, and motoneurons on both sides receive descending input from the same motor cortex. This aberrant descending corticospinal innervation leads to changes in spinal reflex circuits and even in muscle fiber composition. Ultimately, all of these changes cause permanent motor impairment for which no cure and few efficacious treatments currently exist. Nonetheless, many cerebral palsy patients have productive and happy lives and are achieving increasing levels of independence thanks to the advent of adaptive equipment and technology. Although stimulation of primary motor cortex evokes movements, patients typically say nothing as a part of their body moves. This reflects the role of the motor cortex as movement executor but not movement organizer or initiator. Movements evoked by primary motor cortex stimulation range from simple, such as hand-opening or hand-closing, to complex, such as a vocalized cry that requires coordination between the diaphragm, larynx, upper airway, and facial muscles. Both the simple and complex movements are innate in that they are present at birth and do not require learning. On the other hand, actions such as the hand gestures for rock-paper-scissors or the utterance of a word are learned. Thus, the command for volitional actions does not originate in the motor cortex even as the movements are organized for execution there. Consequently, lesions of the primary motor cortex can prevent the execution of learned movements such as rock-paperscissors gestures even though stimulation of motor cortex does not produce these movements. Here, we examine the brain regions that send instructions for volitional actions into the primary motor cortex. They advance an individual toward a goal that is independent of any specific movements or muscles.
Specifications/Details
This syndrome was previously known as thalamic pain syndrome or Dejerine-Roussy disease until it became clear that strokes outside of the thalamus could also produce a similar syndrome of central pain womens health vitamins estrace 1 mg order visa. Central post-stroke pain affects up to 10% of stroke victims and is associated with lesions to ascending pain pathways. Central post-stroke pain is a form of neuropathic pain, which means that no physical stimulus is present and responsible for the pain sensation (see more in Chapter 17). Patients typically perceive a sensation of burning, searing pain in a contralateral distribution. Central post-stroke pain is typically treated with either tricyclic antidepressant or anticonvulsant drugs. These drugs are used at doses that would have little effect on depression or seizures and are thought to decrease pain by blocking burst firing in pain-signaling neurons. Narcotics are typically not used to treat central poststroke pain because they are often ineffective. Other sensory nuclei of the thalamus play similar roles to that of the ventral posterolateral nucleus. For example, damage to the lateral geniculate nucleus impairs contralateral visual perception, rendering the visual world contralateral to the lesion, termed the contralateral visual hemifield (see more later in this chapter), invisible to either eye. However, as described in Chapter 6, unilateral damage to the medial geniculate nucleus does not impact hearing. As a rule, sensory information reaches from the periphery to the cortex in a stereotyped manner: stimulus primary sensory neuron 1 secondary sensory neurons thalamus primary sensory cortex For vision, the basic pathway is: light retinal photoreceptor retinal ganglion cell lateral geniculate nucleus primary visual cortex Despite there being two tracts carrying somatosensory input from the body, somatosensory pathways have a similar organization: touch, vibration, proprioception primary somatosensory afferent dorsal column nucleus ventral posterolateral nucleus primary somatosensory cortex pain and temperature primary somatosensory afferent spinal dorsal horn ventral posterolateral nucleus primary somatosensory cortex One way to view the synapse in thalamus is that it provides a "boost" or a "leg-up," a burst of metabolic and nutritive support for the long journey from here to there. Yet we know that many axons, including dorsal column axons and spinothalamic tract axons, can stretch a meter or more in some individuals. Therefore, it is unlikely that sensory pathways synapse in the thalamus because cortex is too far away for a direct, single axon projection. Rather, as this line of reasoning suggests, the thalamus serves as far more than a relay station. The input from retinal ganglion cells to lateral geniculate neurons comprises well under 5 % of the entire input to these thalamic cells. Thus, in terms of number of synapses, nonlemniscal inputs to thalamocortical projection neurons dominate over lemniscal inputs. Nonlemniscal inputs arise from a variety of brainstem nuclei, cortex, the thalamic reticular nucleus, and from local inhibitory interneurons. The corticothalamic input to thalamocortical projection neurons arises primarily from the same part of cortex to which the thalamic neurons project. Lemniscal inputs and feedback from cortex to thalamocortical projection neurons use the excitatory neurotransmitter glutamate (black). Inputs from the brainstem arise from neurons in nuclei including the dorsal raphe and locus coeruleus, which use a monoamine neurotransmitter. Although inputs from nonlemniscal sources dominate, lemniscal inputs onto thalamocortical neurons carry far more weight than do nonlemniscal inputs.
Syndromes
- Restlessness
- Hives
- Chest pain
- Medicines for motion sickness: dimenhydrinate (Dramamine); meclizine (Bonine, Antivert, Postafen, and Sea Legs)
- If your blood pressure numbers are 120/80 or higher, but below 140/90, it is called pre-hypertension.
- Excessive thirst
Related Products
Additional information:
Usage: ut dict.
Tags: generic 2 mg estrace with mastercard, cheap estrace 2 mg buy on line, trusted 2 mg estrace, buy discount estrace 2 mg on line
10 of 10
Votes: 186 votes
Total customer reviews: 186
Customer Reviews
Torn, 52 years: The dark backing of the eye functions like the darkened interior of a camera: light is absorbed and therefore does not bounce around. As a person hunts and pecks for letters on a keyboard, she is unable to think of much else. Corresponding to the exclusively peripheral vulnerability of hearing, hearing problems, including both deafness and hard of hearing conditions, are classified into two major categories: conductive or sensorineural.
Myxir, 65 years: Ia and Ib afferents are both excited by changes in muscle, but their response characteristics are distinct. In the open configuration (right), ion channels form a pore that allows ions to cross between the cytosol and the extracellular space. Superficial injuries such as a burn, scratch, or a mosquito bite elicit an acute perception of pain (or itch in the latter case).
Ugo, 45 years: In such cases, the working frontal eye fields on the nonlesioned hemisphere shift gaze contralaterally, toward the unaffected side, an effect that is unopposed by the damaged frontal eye fields in the lesioned hemisphere. For any given animal, the capabilities of sensory organs and receptors simply have to match the stimuli that have been important through evolutionary time. Ballism When choreic movements affect the proximal limbs, they appear as large amplitude, repetitive, but constantly varying involuntary movements termed ballism.
Temmy, 21 years: Preganglionic parasympathetic neurons send out long axons that travel to parasympathetic ganglia, which are located in or near the final target tissue. When the membrane potential is depolarized above the resting potential, release of neurotransmitter is increased. The glossopharyngeal nerve serves a hodgepodge of functions, with no single one of them dominating.
Tragak, 59 years: The comorbidity, or coincidence, of anxiety disorders and symptoms reflective of vestibular dysfunction-dizziness, vertigo, disequilibrium, and nausea-may result from the strong influence of vestibular inputs on emotional and homeostatic systems. Thus, tinnitus is linked mechanistically to the loss of hearing; fix the hearing, and the tinnitus will resolve as well. If the patient is a carbon dioxide (C0 2) retainer, you must be cautious when giving oxygen; in this case it is best to limit the initial fraction of inspired oxygen [Fi02) to 0.
Kalesch, 55 years: The movement of outer hair cells serves as an independent resonator, which amplifies the movement of the basilar membrane. The corticobulbar tract forms an analogous pathway to the corticospinal tract, controlling voluntary movement of the face, jaw, tongue, and upper airway along with selected shoulder and neck movements. In most cases, the movements remit completely within several months, either spontaneously or following short-term pharmacological treatment.