- info@careermakers.edu.np
- +977 1 4423870
Furosemide
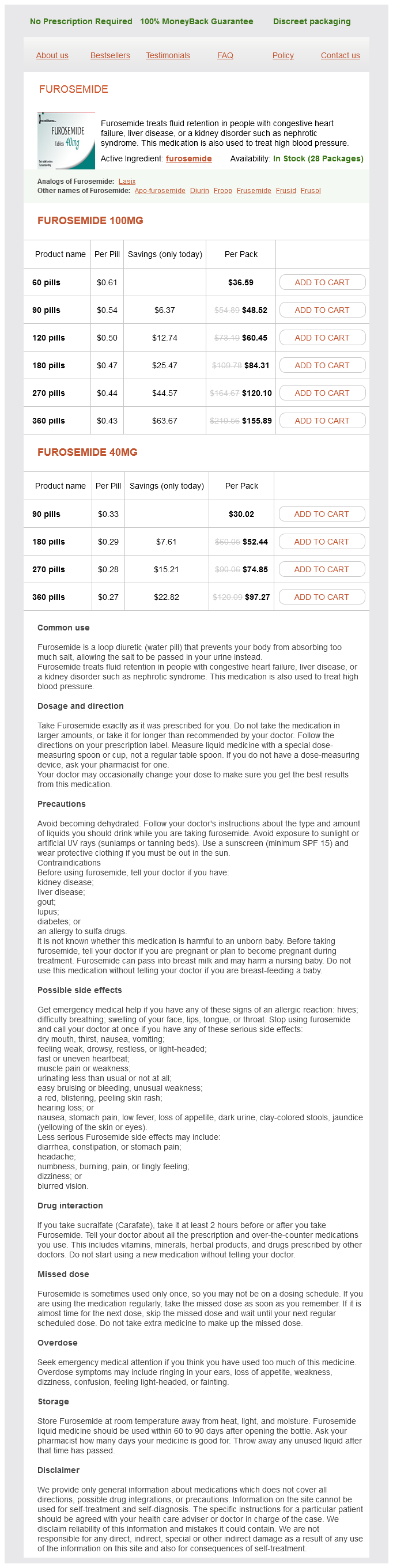
Furosemide 100mg
- 60 pills - $36.59
- 90 pills - $48.52
- 120 pills - $60.45
- 180 pills - $84.31
- 270 pills - $120.10
- 360 pills - $155.89
Furosemide 40mg
- 90 pills - $30.02
- 180 pills - $52.44
- 270 pills - $74.85
- 360 pills - $97.27
Furosemide dosages: 100 mg, 40 mg
Furosemide packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 555
Only $0.29 per item
Description
Treatment may be difficult because surgical excision or radiotherapy cannot completely eradicate a lymphangioma hypertension kidney pathology cheap 40 mg furosemide free shipping. Neuroma,3,6 neurofibroma,34 schwannoma,35 granular cell tumor,36 solitary fibrous tumor,37 myxoma,38 fibroma,39 and other tumors have been reported. Pigmented Lesions of the Conjunctiva Pigmented lesions of the conjunctiva comprise lesions that include melanocytic and nonmelanocytic lesions. These lesions can be challenging for general surgical pathologists due to the unique histologic patterns encountered in the conjunctiva, different from the skin. Proper understanding of the terminologies used by ophthalmologists is necessary to render diagnoses that aid in treatment options. B, D2-40 immunohistochemical stain highlighting the lymphatic channel lining (D2-40 stain, 4×). C, Unilateral conjunctiva lymphangioma in a 33-year-old female with Turner syndrome (H&E, 4×). Racial melanosis may be found in other biopsied lesions of the conjunctiva, including pinguecula, pterygium, squamous papilloma, and squamous intraepithelial neoplasia. Racial melanosis is also very similar to freckles or ephelides, flat patches of epithelial pigmentation concentrated in the basal layer. In congenital ocular melanocytosis or oculodermal melanocytosis (nevus of Ota), episcleral and scleral deeply pigmented dendritic melanocytes with benign cytologic features are present. Acquired conjunctival nevi include compound, junctional, subepithelial, combined, Spitz, inflamed, dysplastic, and pigmented spindle cell nevus. Complexion-associated melanosis is usually observed around the limbus bilaterally, unlike primary acquired melanosis without atypia. It can cover the conjunctiva extensively and the pigmentation may increase with age. B, Melanocytes highlighted with Mart-1 immunohistochemical stain in the cystic compound melanocytic nevus (Mart-1, 10×). C, Conjunctival inclusion cysts highlighted with pancytokeratin immunohistochemistry (pancytokeratin, 10×). Conjunctival nevi present as slightly tan, fleshy, well-defined flat or raised nodules usually located in the interpalpebral bulbar conjunctiva, the plica semilunaris, the caruncle, or the eyelid margin. They are usually darkly pigmented (65% of cases); they may be lightly pigmented (19% of cases) or less frequently nonpigmented (up to 16% of cases). Based on photographic documentation over an average period of 11 years, 13% of benign nevi were found to change in color, and 8% changed in size. Compound melanocytic nevi are the most common type, accounting for 70% to 78% of all nevi. Nesting and a confluent growth pattern of the junctional intraepithelial melanocytic component may be present but is usually limited to the area directly overlying the subepithelial component.
Ruibarbo Caribe (Morinda). Furosemide.
- Are there any interactions with medications?
- Dosing considerations for Noni.
- How does Noni work?
- Are there safety concerns?
- What is Noni?
- Colic, seizures, cough, diabetes, urinary problems, menstrual problems, fever, liver problems, constipation, vaginal discharge, nausea, smallpox, enlarged spleen, kidney disorders, swelling, asthma, bone and joint problems, cancer, eye cataracts, colds, depression, digestion problems, stomach ulcers, heart trouble, high blood pressure, infections, migraine, stroke, pain, reducing signs of aging, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96740
Laryngeal tuberculosis has been reported to occur even in the absence of pulmonary tuberculosis and tends to present with rather nonspecific clinical features heart attack queen order furosemide 40 mg overnight delivery. Initial symptoms of laryngeal tuberculosis include hoarseness, cough, hemoptysis, and dysphagia. The mode of spread to the larynx and trachea is still mostly through expectorated sputum. Although the association of laryngeal tuberculosis with advanced cavitary pulmonary disease is uncommon, most patients with laryngeal tuberculosis also have bacilli in their sputum, still favoring direct pulmonary spread rather than hematogenous seeding. Involvement of the paraglottic space, preepiglottic space, and soft tissue of the anterior neck should be described. Reporting of the neoplasm should include: (1) histologic subtyping, (2) tumor grade, (3) greatest dimension in centimeters, (4) maximum tumor thickness in centimeters, (5) presence of perineural spread, (6) presence of lymphovascular invasion, (7) invasion of cartilage or ossified cartilage, (8) multicentric invasive carcinoma, (9) diffuse/multicentric carcinoma in situ, and (10) any additional pathology noted (squamous papilloma, inflammatory changes, bacteria or fungi noted, etc. Status of the inked resection margins should include a measurement of the closest margins in millimeters, if possible, and should note the presence of high-grade dysplasia at the margin when pertinent. The endoscopic laser resection for low-stage laryngeal carcinomas presents a new paradigm with respect to resection margins. These specimens may be removed and submitted piecemeal, and the surgeon may laser through the carcinoma during the procedure. There is nodular surface irregularity with destruction of the normal surface anatomic landmarks. B and C, Subepithelial stroma contains granulomas (B) with Langhans-type giant cells (C), histiocytes, and lymphocytes. Early infection may be histologically nonspecific, with an acute inflammatory infiltrate and a lack of well-formed granulomas. The diagnosis of tuberculosis requires a Ziehl-Neelsen stain and patience, as one might have to examine many step sections to find a solitary "red snapper. Normal laryngeal mucosa rarely harbors significant inflammation; therefore any moderate to severe acute and/or chronic inflammation should be viewed as pathologic, and the possibility of infection should be considered. Apart from tuberculosis, granulomatous inflammation in the larynx can be seen in some other rare infections, such as in coccidiodomycosis, cryptococcosis, blastomycosis, and leprosy. Tuberculoid leprosy can be distinguished from tuberculosis as leprosy may involve nerves, which is uncommon for tuberculosis, and M. Granulomata in sarcoidosis are characteristically nonnecrotizing, although, rarely, necrosis may be present. Laryngeal tuberculosis must be distinguished from foreign bodytype granulomatous inflammation in the larynx, which can be seen after Teflon injection or with laryngeal amyloidosis.
Specifications/Details
However arrhythmia uti buy furosemide 100 mg mastercard, with small biopsies, this differential diagnosis may be problematic and immunohistochemistry can be helpful. The treatment of choice is complete surgical excision, partial or complete laryngectomy, plus adjuvant radiotherapy. However, a recent series showed that radiation therapy may also be used primarily to avoid a total laryngectomy or after laryngeal preservation surgery, with excellent local control rates and preservation of laryngeal function and voice. Isolated pulmonary metastasis should be treated aggressively and not alter treatment of the primary tumor. Some patients may have rapid disease progression or acceleration to a more rapid clinical course. Tumors usually originate in the submucosa and may be as large as 5 cm in greatest dimension. They have an appearance similar to that of their salivary gland counterpart, are composed of clear, mucin-secreting, intermediate, and squamous-like cells, in varying proportions arranged in solid or cystic nests (for a detailed histologic description, refer to Chapter 6). Occasional tumors may arise from surface mucosa; a clear cell variant has also been reported. Organ conservation is the preferred approach using laser treatment,540 but partial or total laryngectomy may be indicated. In high-grade tumors, recurrence is more common and radical surgery with radiotherapy is recommended (for more specific information about survival, see Chapter 6). Mucosal melanoma comprises less than 2% of all Western melanomas542 and represents 4% of malignancies arising from nasal cavity and paranasal sinus. In a recent update, the most frequently affected regions were supraglottis (60%) and glottis (40%). Clinically, mucosal melanomas appear as brown, tan, or bluish polypoid tumors, but in some patients, melanoma can present with dark discoloration of the supraglottic larynx and incomplete mobility of the vocal fold. Macroscopically, mucosa/laryngeal melanoma presents as a nodular neoplasm arising from the mucosa. The detection of in situ components is more difficult in upper aerodigestive tract mucosa because of the thinness of the surface epithelium and frequent ulceration. Plasmacytoid melanomas have nuclei that are eccentric and cytoplasm that is bright pink to dirty brown and granular. Intranuclear vacuoles or holes or pink nucleoli are helpful giveaways to the true diagnosis. Spindle cell melanomas can mimic a sarcoma, and the nuclei often have a variable morphology. Epithelioid melanoma forms sheets of large plump cells that have a nesting tendency. Intranuclear vacuolations are seen, and, again, melanin pigment may be seen in the cytoplasm. However, one should remember that the majority of mucosal melanomas are amelanotic.
Syndromes
- Possible foreign object in the airway
- Syphilis, a sexually transmitted infection
- Inflammation of the aorta (aortitis) with aortic aneurysm
- Low blood pressure
- Make sure the all information is filled in clearly.
- Wheezing
- No urine output
- Vision disorders
- Shortness of breath
Related Products
Additional information:
Usage: p.c.
Tags: buy furosemide 100 mg low price, furosemide 100 mg purchase free shipping, furosemide 40 mg buy, furosemide 100 mg with visa
9 of 10
Votes: 105 votes
Total customer reviews: 105
Customer Reviews
Tukash, 34 years: Hematogenous metastatic disease, usually pulmonary, has been reported; survival is short after the development of metastases. The atrophic variant of dermatofibrosarcoma protuberans in childhood: a report of six cases.
Garik, 36 years: Low-grade myofibroblastic sarcoma, which frequently involves the head and neck, may be extremely difficult to distinguish from nodular fasciitis. The cells in this tumor closely mimic the ameloblasts and stellate reticulum of the developing tooth organ.
Volkar, 52 years: This feature has been demonstrated in serial biopsies showing progressive maturation to a lesion consisting of lamellar bone in a moderately cellular fibrous stroma. Therefore, the thyroid affected by Hashimoto thyroiditis is not adherent to the surrounding soft tissues of the neck.
Sibur-Narad, 40 years: However, hospital staff have developed Coccidioidomycosis after removing a plaster cast from a patient with Coccidioides osteomyelitis caused by germination within the cast. However, scrofula (suppurative, draining cervical mycobacterial lymphadenitis) may occur.
Nefarius, 48 years: The rarity of these tumors precludes definitive recommendations regarding management and prognosis. It is relatively common to see a mild degree of nuclear pleomorphism and enlargement in otherwise typical granular cell tumors.