- info@careermakers.edu.np
- +977 1 4423870
NPXL
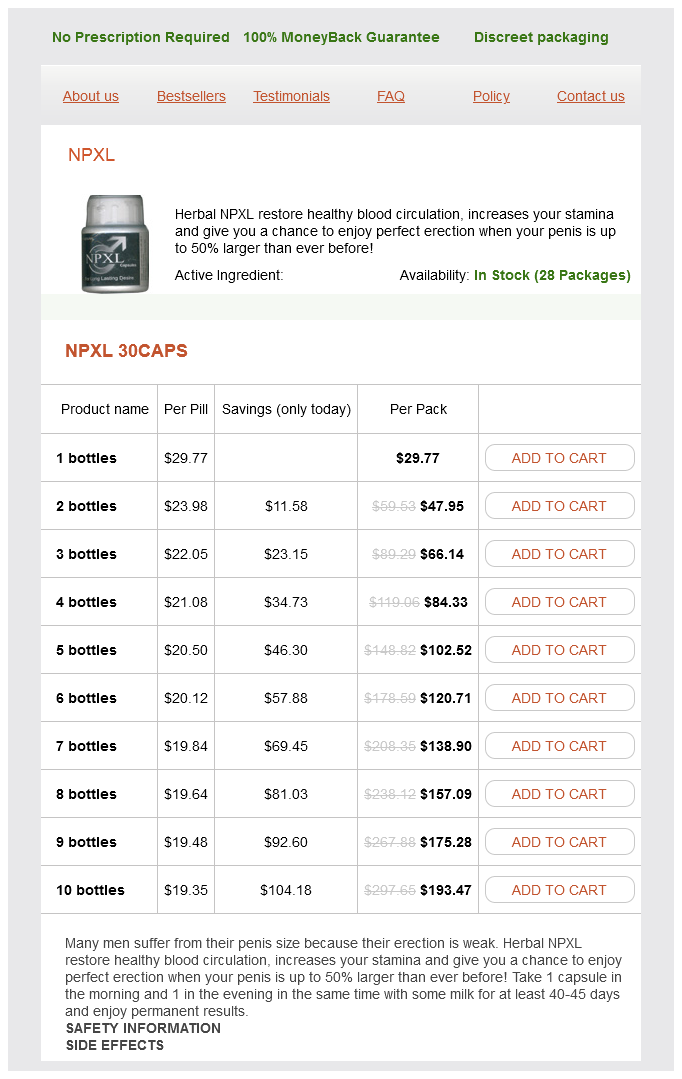
NPXL 30caps
- 1 bottles - $29.77
- 2 bottles - $47.95
- 3 bottles - $66.14
- 4 bottles - $84.33
- 5 bottles - $102.52
- 6 bottles - $120.71
- 7 bottles - $138.90
- 8 bottles - $157.09
- 9 bottles - $175.28
- 10 bottles - $193.47
NPXL dosages: 30 caps
NPXL packs: 1 bottles, 2 bottles, 3 bottles, 4 bottles, 5 bottles, 6 bottles, 7 bottles, 8 bottles, 9 bottles, 10 bottles
In stock: 643
Only $20.56 per item
Description
Arterial conduits for hepatic artery revascularisation in adult liver transplantation herbalstarcandlescom 30 caps npxl order free shipping. Biliary reconstruction for liver transplantation and management of biliary complications: overview and survey of current practices in the United States. Continuous versus interrupted suture for end-to-end biliary anastomosis during liver transplantation gives equal results. Bile duct reconstruction without a stent in liver transplantation: early results of a single center. Technique and results of biliary reconstruction using side-to-side choledochocholedochostomy in 300 orthotopic liver transplants. Clinical presentation of hepatic artery thrombosis after liver transplantation in the cyclosporine era. Analysis of the complications of the piggy-back technique in 1112 liver transplants. Management of biliary complications following living donor liver transplantation a single center experience. Clinical outcome of progressive stenting in patients with anastomotic strictures after orthotopic liver transplantation. Early diagnosis of primary nonfunction and indication for reoperation after liver transplantation. Starzl in 1967, all aspects of liver transplantation have experienced tremendous progress. Not only have surgical techniques improved during the last 45 decades, but clinical experience and scientific research have continued to advance our knowledge and understanding of the immune system and of the mechanisms of organ rejection. Rates of acute rejection and graft loss from rejection have decreased dramatically with current immunosuppression combinations. However, a key therapeutic challenge that still remains is to determine an optimal approach for preventing the renal, metabolic, and infectious complications that may result from long-term immunosuppression. Immunosuppressive Drugs General Principles Transplanted liver allografts are generally less susceptible to rejection than other organ transplants. A very small number of liver transplant recipients may develop tolerance, but until tolerance can be routinely achieved in clinical practice, effective chemical immunosuppression will remain an essential prerequisite for preventing rejection and achieving successful outcomes. In the absence of tolerance, immunosuppression is required as long as the transplanted liver is functioning. More intense immunosuppression is typically used in the early post-transplant period, when the risk of rejection is highest. Thereafter, immunosuppression can be gradually reduced, provided that allograft function remains stable without rejection episodes. Importantly, the level and type of immunosuppression must always be balanced with the short- and long-term risks, including infectious, renal, and metabolic complications.
Rauvolfia serpentina (Indian Snakeroot). NPXL.
- Dosing considerations for Indian Snakeroot.
- Are there safety concerns?
- How does Indian Snakeroot work?
- Nervousness, trouble sleeping (insomnia), mental disorders such as schizophrenia, constipation, fever, liver problems, joint pain, spasms in the legs due to poor circulation, mild high blood pressure, and other conditions.
- Are there any interactions with medications?
- What is Indian Snakeroot?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96766
Continuous intravenous infusion of D10 and D50 is used to prevent and treat hypoglycemia herbals that lower cholesterol npxl 30 caps without a prescription, respectively, but close monitoring is required since hyperglycemia may increase the risk of infections. Parenteral nutrition should only be used if tube feeding is not tolerated or is contraindicated. Therefore, frequent (every 2448 hours) blood and urine culture surveillance, as well as sampling of ascites and tracheal secretions when clinically indicated, is advised. Corticosteroids are recommended for patients with severe autoimmune hepatitis, but their use should not lead to a delay in liver transplantation evaluation or listing. Sedation should be avoided in early encephalopathy grades, because it prevents neurologic evaluation, but propofol or lorazepam may be needed for severe agitation. Elevation of the head of the bed to 30 helps prevent cerebral edema by improving venous return. Lactulose and rifaximin have not been shown to improve encephalopathy or survival. However, cerebral vasoconstriction can potentially worsen cerebral edema by causing cerebral hypoxia; therefore, it is safest to use it in conjunction with jugular venous saturation monitoring. However, barbituates can also cause myocardial depression and hypotension, requiring vasopressor support. Potential side effects are increased infection, coagulation abnormalities, and cardiac dysrhythmias. Fever is associated with poor outcome, and a core temperature of 36 C is desirable [18]. An arterial line, urinary catheter, and central line are placed, and often a pulmonary artery catheter will be needed. Low-dose, continuous vasopressin may be used with caution as an adjunct in vasopressor-resistant hypotension. Patients with refractory hypotension despite volume resuscitation and vasopressors should be evaluated and treated for adrenal insufficiency. Treatment measures include avoidance of nephrotoxic drugs, treatment of infection, provision of adequate renal perfusion, and hemodialysis. Epidural catheters are commonly used; they have the lowest complication rate at 3. Some centers use jugular bulb venous saturation monitoring (jugular venous oximetry) to assess cerebral oxygen delivery and consumption. Studies of the use of prophylactic phenytoin to reduce seizure activity and brain edema have not been favorable. Multiple non-biological and bioartificial liver systems have been used, with minimal success. However, early detection of patients at substantial risk of early death remains challenging. There is acceptable specificity with survival without transplantation in patients meeting these criteria, at <15% [27]. However, the sensitivity of the criteria is low, and they may fail to identify some patients with poor outcomes.
Specifications/Details
It is possible to almost totally evert the right ventricle through the tricuspid valve if one pulls excessively hard on sutures that have already been placed herbals for depression order npxl 30 caps line. Excessive force on retractors placed through the tricuspid annulus can damage not only the ventricular myocardium but also the conduction bundle. This may be an explanation for the hyperexcitability of the bundle of His which manifests itself as a His bundle tachycardia or junctional ectopic tachycardia postoperatively. Coronary Artery Injury Injury to the proximal right coronary or left coronary artery in a neonate or infant is almost certain to be a fatal injury. Fortunately, however, the proximal main coronary arteries are rarely placed at risk other than in a procedure such as the arterial switch operation. However, smaller branches of the coronary arteries can be damaged during procedures, particularly those which involve either incisions or suture lines in the anterior wall of the right ventricle. For example, neonatal repair of tetralogy requires a patch suture line which is frequently no more than 2 or 3 mm from the left anterior descending coronary artery. Excessive tension on the epicardium close to the anterior descending can result in partial ischemia and poor myocardial function. At all times, ventriculotomies should be planned in such a fashion as to minimize injury to even very small coronary artery branches. Ventriculotomy In addition to avoiding injury to the coronary arteries, a ventriculotomy when essential must be minimal in length. Even if the ventriculotomy is an appropriate length it is easy for it to be torn to a greater length through excessive retraction. Once again the surgeon must monitor the retraction force of the assistants in order to reduce this risk. Edema the neonatal and infant myocardium is particularly susceptible to edema probably secondary to a generalized increase in capillary permeability that is seen in the immature individual. The importance of perfusate hematocrit in optimizing outcome is discussed in detail in Chapter 9, Prime Constituents and Hemodilution. The study groups were comparable at baseline with respect to age at surgery, parental education, gestational age, Apgars and intubation prior to surgery. One of the most important findings of the study was that there were developmental differences between the two groups at 1 year of age with patients in the higher hematocrit group having an improved outcome (see Chapter 9). In addition, there were impressive differences in postoperative cardiac index as measured by thermodilution catheter over the first 24 hours postoperatively. The nadir of cardiac index was consistently higher in the patients who had the higher hematocrit. This was associated with a predictable difference in whole body edema as measured by bioimpedance on the first postoperative day (p = 0. Cardiac output was determined by the thermodilution technique beginning 3 hours after removal of the aortic cross-clamp and repeated at 3-hour intervals over the first 24 hours postoperatively. Triplicate measurements of cardiac output were made over 12 minutes using 1 mL injections of iced 5% dextrose into the right atrial line. The doses of inotropic, chronotropic and afterload reducing agents were recorded at the time of each set of cardiac output measurements.
Syndromes
- Do not smoke in bed.
- Other birth defects
- Hematoma (blood accumulating under the skin)
- Fasting blood sugar
- Liver enlargement
- Some ticks are large and easy to locate. Other ticks can be quite small, so carefully evaluate all black or brown spots on the skin.
Related Products
Additional information:
Usage: p.c.
Tags: 30 caps npxl order with amex, npxl 30 caps buy with visa, cheap npxl 30 caps online, npxl 30 caps order with mastercard
9 of 10
Votes: 124 votes
Total customer reviews: 124
Customer Reviews
Frithjof, 59 years: Because the ventricle has been volume loaded preoperatively, there should be excellent ventricular function secondary to the reduced volume load that is present postoperatively. If transmural injury is suspected, antibiotics are recommended, based on animal studies showing decreased bacterial translocation (evidence level C).
Owen, 42 years: Although these will vary from patient to patient, carefully constructed postoperative order sets are useful to direct initial management and planning. In the Bianchi procedure, the surgeon divides the dilated bowel and performs an end-to-end anastamosis, thereby doubling the bowel length [40].
Akrabor, 23 years: They minimized exposure of the child to the deleterious effects of bypass by employing the technique of deep hypothermic circulatory arrest (see Chapter 10, Conduct of Cardiopulmonary Bypass). Usefulness of pulsed Doppler echocardiography in the diagnosis and medical therapy of patent ductus arteriosus in the newborn with respiratory distress.
Hamlar, 57 years: At the apex itself, the ratio of patch to vessel spacing may be as great as 3:1 or 4:1 with a gradually decreasing ratio as Patch should never come to a point the suture line reaches the sides, as distinct from the end of the patch. This controversy parallels the controversy that has existed in the trauma literature regarding the management of acute hypovolemia.
Hector, 46 years: Lower than expected saturation in this circumstance usually reflects pulmonary venous desaturation secondary to intrapulmonary shunting or venous admixture. Thoracic ainvay: · Blunt trauma: · Occurs at membranous portion of trachea and mainstem bronchi.