- info@careermakers.edu.np
- +977 1 4423870
Tenormin
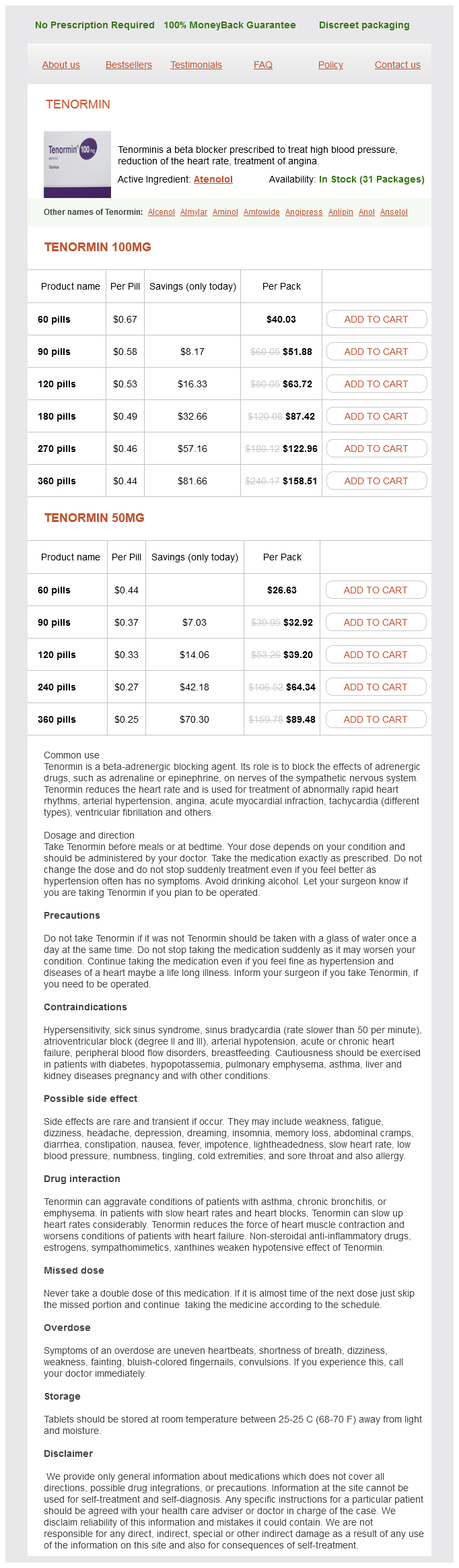
Tenormin 100mg
- 60 pills - $40.03
- 90 pills - $51.88
- 120 pills - $63.72
- 180 pills - $87.42
- 270 pills - $122.96
- 360 pills - $158.51
Tenormin 50mg
- 60 pills - $26.63
- 90 pills - $32.92
- 120 pills - $39.20
- 240 pills - $64.34
- 360 pills - $89.48
Tenormin dosages: 100 mg, 50 mg
Tenormin packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills, 240 pills
In stock: 842
Only $0.26 per item
Description
Supportive treatment includes correction of fluid and electrolyte imbalance arrhythmia interpretation purchase 50 mg tenormin otc, blood (or exchange) transfusion, administration of oxygen by mask and adequate analgesics for pain relief. Complications include cardio-respiratory failure and thrombo-embolism and hence thromboprophylaxis needs to be administered. Multidisciplinary team input with the involvement of anaesthetists, haematologists and physicians may be necessary. Aortic dissection or rupture Aortic dissection is a rare but potentially life-threatening condition that may be easily missed during pregnancy as illustrated in our case discussion. Aortography is no longer the gold standard as it is invasive and involves injection of a dye. Upper abdominal pain radiating to the back, predominantly back pain or sharp stabbing pain in the centre of the chest or abdomen should raise suspicion. Complications include myocardial infarction, ischaemic bowel syndrome, peripheral neuropathy, paraplegia and cardiorespiratory arrest. Urgent cardiothoracic surgery is indicated, especially in cases of proximal aortic dissections involving the ascending aorta. Surviving sepsis campaign guidelines for management of severe sepsis and septic shock. Conclusion Common causes for abdominal pain during pregnancy include round ligament strain, symphysis pubis diathesis and musculoskeletal disorders. However, it is important to appreciate that several life-threatening obstetric and other intra and extraabdominal conditions may present with acute abdominal pain. Pregnancy may also mask or alter clinical presentation of serious intra-abdominal conditions like acute appendicitis and pancreatitis leading to a delay in diagnosis. Emergency surgery is indicated for acute abdomen, as in the non-pregnant state, as a delay in treatment may increase maternal morbidity and mortality. It is also important to recognise that rare extra-abdominal conditions such as dissection or rupture of the ascending aorta can also present with upper abdominal pain. Acute abdomen refers to an intra-abdominal process that is characterised by abdominal pain, tenderness and muscular rigidity, for which emergency surgery must be considered. Rare causes such as pulmonary embolism, myocardial infarction and aortic dissection may present with upper abdominal pain and backache. A Gravid uterus may mask the signs of peritoneal irritation (guarding, rigidity and rebound tenderness) by preventing the contact between the parietal peritoneum of the anterior abdominal wall and the inflamed organ. Radiological investigations, including abdominal X-rays, can be safely undertaken during pregnancy and should be always considered so as to avoid failures in diagnosing potentially lifethreatening conditions. This review will summarise the latest literature and discuss the management for pre-existing diabetic women during pregnancy. There is a higher incidence of stillbirth, macrosomia and congenital malformations. Pre-pregnancy counselling is essential to prepare for pregnancy, to tighten glycaemic control and review medication prior to pregnancy.
PLE (Pomegranate). Tenormin.
- Dosing considerations for Pomegranate.
- How does Pomegranate work?
- What is Pomegranate?
- Chronic lung disease (chronic obstructive pulmonary disease, COPD).
- Are there any interactions with medications?
- Are there safety concerns?
- High cholesterol (hyperlipidemia), heart disease, intestinal worm infestations, high blood pressure (hypertension), hardening of the arteries (atherosclerosis), obesity and weight loss, gum disease, fungal mouth infections, diarrhea, dysentery, sore throat, hemorrhoids, prostate cancer, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96406
Influenza vaccination administered in pregnancy has also been shown to confer immunity to the neonate arteria renalis dextra 100 mg tenormin purchase with visa. Novel influenza A (H1N1) virus in pregnancy: the most frequently reported symptoms among non-pregnant patients with swine fever have been fever, cough, and sore throat. The number of severe cases was significantly less, the earlier oseltamivir was started after onset of symptoms. Severe and moderate cases occurred in all trimesters but the highest numbers were seen in the third trimester. Six women died e all were women who developed pneumonia and subsequent acute respiratory distress syndrome requiring mechanical ventilation. Hence recommendations are that pregnant women with confirmed, probable, or suspected H1N1 virus should receive a 5 day course of antiviral treatment ideally from within 48 hours of symptom onset. Oseltamivir should be considered the preferred treatment for pregnant women because its higher systemic absorption might suppress influenza viral loads more effectively in sites other than the respiratory system. Pregnant women in close contact with a confirmed, probable, or suspected case should receive a 10-day course of prophylaxis with zanamivir or oseltamivir. Those women who do develop clinical varicella should be treated with acyclovir and intravenous therapy may be necessary. Maternal and neonatal morbidity and mortality in cases of maternal varicella pneumonia justifies the use of i. A study has suggested that later gestational age (perhaps because of increased immunosuppression) at the onset of varicella pneumonia is a significant risk factor for maternal mortality. Anyone with varicella should be examined at a distance from the antenatal clinic and ward to minimize exposure to other pregnant women. It should be suspected in the presence of profound hypoxia out of proportion to the chest X-ray findings and bronchoscopy should be considered. Clinical varicella after 20 weeks gestation: oral acyclovir (800 mg five times a day for 7 days) if within 24 hours of the onset of the rash. Aim to avoid delivery and provide supportive treatment and intravenous acyclovir - however, delivery may be required in women to facilitate assisted ventilation in cases complicated by respiratory failure. The patient is often asymptomatic but typically can present with a cough, haemoptysis, weight loss and night sweats. The diagnosis is confirmed with sputum examination for acid-fast bacilli (ZiehleNeelsen stain). In the event that the transaminases more than double, all antituberculous chemotherapy should be temporarily withdrawn and then individual agents introduced in a step-wise fashion while liver function tests are monitored closely. Since rifampicin induces the enzyme cytochrome P450, vitamin K should be given to the mother in the same way it is given to mothers receiving enzyme-inducing antiepileptic drugs. After delivery the neonate should be given prophylactic isoniazid treatment if the mother is sputum positive and vaccinated as soon as possible. Breastfeeding is not contraindicated since very little of the drugs are excreted in breast milk. Extrapulmonary disease (at sites such as lymph nodes, bone, liver, spleen, bone marrow, caecum, nervous system and eye) was as common as pulmonary disease in pregnancy with a greater delay in diagnosis.
Specifications/Details
Many of these deaths are attributable to uterine rupture heart attack cough discount 50 mg tenormin visa, due to a prolonged, unattended obstructed labour. In resource rich countries, effective antenatal and intrapartum care has almost eradicated this condition as a cause of maternal death. The incidence of uterine rupture is increased amongst those who are multiparous and live in remote regions. In such settings the incidence of uterine rupture may be as high as 1:69 deliveries (rural Nigeria). The main reason for the discrepancy between the maternal mortality from obstructed labour in resource rich and resource poor countries is lack of access to functional maternity services (including skilled birthing attendants), lack of access to safe operative delivery, and late presentation to functional maternity services. The use of partograms for recognition of abnormal labour is one cheap strategy that could potentially facilitate a standard of labour management in resource poor countries. For example, rural centres employing a standard partogram could recognize obstructed labour at an earlier stage. This strategy, whilst promising, needs to be introduced and used in a culturally acceptable manner, and will only work when there are adequate trained birth attendants to assess women in labour, and adequate infrastructure to organise timely transfer to larger centres which have the resources to provide safe operative delivery. Unsafe abortion the rate of maternal death from unsafe abortion is significantly higher than for abortion in an appropriate medical setting. Ninety-nine percent of deaths that occur as a result of abortion are from unsafe abortion, provided by unskilled providers in unsterile conditions. Determining a true estimate of maternal deaths from abortion is inherently challenging. Not surprisingly, the incidence of unsafe abortion correlates with the restrictiveness of abortion law, and as a result procurement of abortion will be under-reported in countries with the highest rates of unsafe abortion. Improving access to effective, culturally acceptable contraception is key to reducing unwanted pregnancy. However, no contraception is entirely effective, and access to safe abortion will remain crucial to reducing maternal mortality. This will be difficult to achieve in countries where entrenched beliefs influence the law and override the right of women to access safe medical services. Although the maternal mortality rate was not affected by the introduction of measures to prohibit abortion in countries such as Chile, El Salvador and Nicaragua, the obvious rebuttal to this is that the rates of maternal mortality due to abortion may be under-reported where the practice is illegal. Making abortion services illegal does not reduce the rate at which women seek abortion, but it does reduce the rate of safe abortion, and increase the rate at which women die from abortion. Reducing maternal mortality the World Health Organization has published a list of the interventions that are the desirable standard, and should be available to all women during pregnancy, delivery and postpartum Table 1). These interventions are more easily accessible in resource rich countries, where almost every woman has at least four antenatal care visits, is attended by a skilled health worker during childbirth and receives postpartum education and follow-up. In order to improve maternal mortality in resource poor countries, we need to identify and remove the barriers that limit access to health services.
Syndromes
- Strain
- Botulinum toxin to help with spasticity and drooling
- Poor feeding
- Does breathing difficulty cause you to wake up at night (paroxysmal nocturnal dyspnea)?
- Cimetidine
- You will be screened for alcohol and tobacco use and for depression.
- Change positions often, at least every 2 hours
- Gram stain, other special stains, and culture of CSF
Related Products
Additional information:
Usage: p.c.
Tags: generic tenormin 50 mg without a prescription, generic tenormin 50 mg overnight delivery, generic tenormin 100 mg without prescription, generic tenormin 50 mg buy
8 of 10
Votes: 244 votes
Total customer reviews: 244
Customer Reviews
Zarkos, 53 years: The placenta and membranes should always be examined carefully after delivery to ensure that they are complete. Progesterone Progesterone has been of interest for the prevention of preterm labour for many years. Recipients of kidneys from older living donors have a better survival than recipients of kidney from young deceased donors.
Fedor, 24 years: Most of the conditions requiring advanced work-up should be referred to a pediatric nephrologist or urologist. Although usually undesirable, this may be of clinical benefit in certain circumstances, for example improving uteroplacental blood flow in pre-eclampsia. Although prophylactic administration of an antimicrobial agent limited to a period when a person is at high risk of otitis media has been suggested (eg, during acute viral respiratory tract infection), this method has not been evaluated critically.