- info@careermakers.edu.np
- +977 1 4423870
Viagra Professional
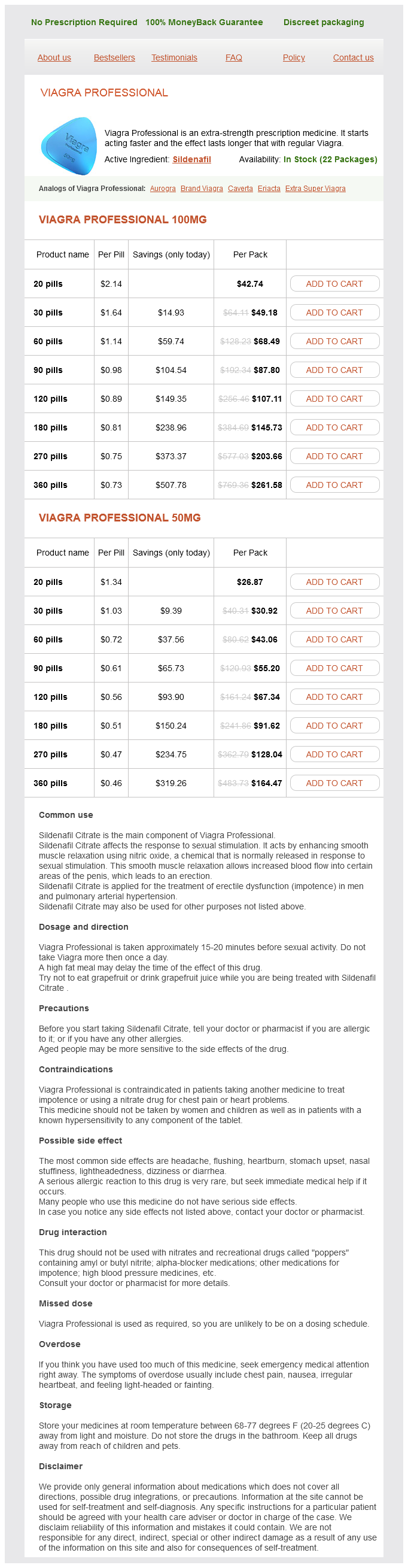
Viagra Professional 100mg
- 20 pills - $42.74
- 30 pills - $49.18
- 60 pills - $68.49
- 90 pills - $87.80
- 120 pills - $107.11
- 180 pills - $145.73
- 270 pills - $203.66
- 360 pills - $261.58
Viagra Professional 50mg
- 20 pills - $26.87
- 30 pills - $30.92
- 60 pills - $43.06
- 90 pills - $55.20
- 120 pills - $67.34
- 180 pills - $91.62
- 270 pills - $128.04
- 360 pills - $164.47
Viagra Professional dosages: 100 mg, 50 mg
Viagra Professional packs: 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 918
Only $0.49 per item
Description
Blood is supplied to the condyles by a branch of the digital artery and vein that travels with the collateral ligaments erectile dysfunction drugs in canada cheap viagra professional 50 mg buy online. Care must be taken not to disrupt this blood supply or to strip small fragments of their soft tissue attachments. The mechanism is hypothesized to be tension or rotation force through the collateral ligaments for an oblique fracture and compression and subluxation in the case of a coronal fracture. Table 1 Fracture Configuration Type I: unicondylar short oblique Condylar Fracture Patterns Fixation Illustration Characteristics Unstable Fracture exits just proximal to collateral ligaments Deformity is oblique to coronal and sagittal planes Nondisplaced Fracture Could consider nonoperative treatment, but must follow closely. Joint subluxation is an absolute indication for surgery and must be assessed carefully both radiographically and clinically. Most commonly, the condyle toward the midline of the hand (ie, the middle finger axis) is fractured: the ulnar condyle in the index finger and thumb and the radial condyle in the ring and small fingers. Weiss et al5 found five of seven nondisplaced fractures treated conservatively went on to displace and required surgery. Also, with close follow-up, if a fracture were to displace later, it could be addressed at that point, although it would require slightly more work to regain reduction and functional restoration. On the other hand, there is minimal morbidity in percutaneous pinning, and that would minimize the likelihood of displacement in a fracture that often is unstable. Several review texts suggest that coronal fractures of less than 25% of the joint surface with a stable congruent joint can be treated nonoperatively or with fragment excision. Although this may be true, there are few biomechanical or clinical outcomes data to support the statement. Fracture reduction, implant placement, and fracture stability are effectively evaluated fluoroscopically. The lateral (mid-axial) approach is suggested as a means to minimize extensor mechanism scarring, but only if significant joint incongruity or comminution is absent. A bicondylar or triplane fracture requires a more global joint and fragment exposure. The extensor tendon may be split longitudinally, but preferably incisions are made on its borders, allowing mobilization and excellent joint exposure. If necessary, make a Brunner-style volar incision, and retract the flexor tendons to expose the volar plate. If possible, reflect the volar plate on one side and a little up the lateral edge for exposure via a triangle-shaped flap. If more complete exposure is needed, make a transverse incision along the proximal edge of the volar plate, leaving enough proximal cuff to reattach the volar plate. Elevate the volar plate on a distal hinge, repair the fracture, and then reattach the volar plate. Avoid at all costs stripping soft tissue attachments from small fracture fragments. Fracture displacement typically is in an oblique plane, sometimes not well appreciated on the straight anteroposterior or lateral views.
Kamillen (German Chamomile). Viagra Professional.
- Is German Chamomile effective?
- Are there any interactions with medications?
- What is German Chamomile?
- Treating or preventing swelling and deterioration (mucositis) of the mouth lining caused by radiation therapy and some types of chemotherapy.
- Dosing considerations for German Chamomile.
- Colic in breastfed infants when used in combination with other herbs.
- What other names is German Chamomile known by?
- How does German Chamomile work?
- Upset stomach (dyspepsia), when a combination of German chamomile and five other herbs is used.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96914
Therefore erectile dysfunction relationship discount viagra professional 50 mg with visa, a limb-sparing tumor resection at that site begins with dissection and preservation of the superficial femoral vessels. Large high-grade sarcomas usually necessitate ligation of the profundus femoris artery. The surrounding adductors are then detached from their origin along the inferior and superior pubic rami and ischium and removed en bloc with the tumor. The soft tissue defect remaining after tumor resection is usually reconstructed by transferring the sartorius muscle and the remaining medial hamstrings. The bony structures of the pelvic floor are the closest margins for large sarcomas that arise within this muscle group. Rarely, proximal adductor tumors may extend as a dumbbell around the ischium into the ischiorectal fossa. There is no intermuscular septum separating the adductor group from the posterior hamstrings proximally; therefore, extracompartmental extension may occur between the adductor muscles and the medial hamstrings as these tumors enlarge proximally. In those cases, we recommend induction chemotherapy or isolated limb perfusion and repeated staging studies before a definitive decision is made regarding amputation. The profundus femoris artery, on the other hand, is often involved and must be ligated as it passes through the adductor brevis. The obturator artery and nerve, which pass through the obturator fascia, are routinely ligated. In light of the above, preoperative vascular evaluation of the patient should include direct questioning about intermittent claudication, limb swelling, and deep vein thrombosis. Compartmental muscles arise from the pelvic floor and the medial aspect of the ipsilateral pelvic ring (symphysis pubis, inferior pubic ramus, ischium, and obturator fascia) and attach distally to the linea aspera and the medial aspect of the distal femur. The superficial femoral artery passes along the anterior and lateral margins of the entire compartment and forms the lateral border. Coronal section showing a dumbbell-shaped extension around the ischium into the pelvic cavity. Although the vessels are considerably displaced, a plane of dissection is evident between them and the tumoral mass. Biplanar angiography, especially in patients older than 40, should be done to evaluate the patency of the superficial femoral artery: ligation of the profundus artery without a patent superficial femoral artery will lead to a nonviable extremity. In the past, angiography was also used preoperatively to outline the course of the vascular bundle within the affected thigh and to assess the likelihood of vascular reconstruction. This incision permits large anterior and posterior flaps to be developed to visualize the vastus medialis, the sartorial canal, and the entire adductor compartment. The sartorial canal is opened proximally to identify the common femoral artery before ligating the profundus vessels.
Specifications/Details
Origins of the vastus lateralis young erectile dysfunction treatment viagra professional 100 mg without a prescription, vastus intermedius, and vastus medialis on the femur are transected from bone by using electrocautery. Using strong upward and medial traction on the specimen, the insertions of the vastus lateralis, vastus medialis, and rectus femoris into the patellar tendon are divided on the patella bone. The dissection site is copiously irrigated, and any bleeding points are secured with ligatures or electrocautery. To facilitate rehabilitation by helping to provide stability to the knee, the gracilis muscle medially and the short head of the biceps muscle laterally are transected at their insertions on the medial and lateral collateral ligaments. This transection should be as far distal as possible so that a tendinous portion of the muscle is retained. Then, using heavy nonabsorbable sutures, these two muscles are transplanted onto the patellar tendon. The muscles are approximated in the midline to cover the distal third of the femur. Suction catheters are placed beneath the skin flaps and the subcutaneous tissue is approximated. The skin is closed and the incision is covered with povidoneiodine ointment and a loose dry sterile dressing. The patient may begin ambulation when the suction catheters have been removed and edema of the leg has resolved. Because the lymphatics along the superficial femoral artery and within the buttock remain intact, prolonged swelling is not usually a problem, serous drainage from transected muscle bundles does not occur in large amounts. Several millimeters of the outer cortex can be removed; however, the outer cortex itself should not be removed en bloc. Suction catheters are placed beneath the skin flaps and the subcutaneous tissue is approximated with interrupted absorbable sutures. Another technique that can be used to functionally reconstruct large defects (which is not within the scope of this textbook) is latissimus dorsi microvascular transplantation. This transection should be as far distal as possible to retain a tendinous portion of the muscle. The muscle is transferred anteriorly to the midline so that it will have an almost direct line of pull. Then, using heavy, nonabsorbable sutures, the muscle is transplanted onto the patella and the remains of the quadriceps tendon and rectus femoris. Sartorius Muscle Transfer Semitendinosus Muscle Transfer the muscle is transected as far distal as possible from its insertion to the proximal tibia and transferred anteriorly so that it will have an almost direct line of pull. The muscle and its tendinous part are then sutured to the patella and the remains of the quadriceps. After completion of the resection, the sartorius muscle is released, but not transected, from its distal insertion on the medial aspect of the proximal tibia.
Syndromes
- Itching, burning skin, or rash
- Arsenic poisoning may cause white lines and horizontal ridges.
- Connective tissue diseases such as rheumatoid arthritis or systemic lupus erythematosus (the most common cause in children)
- Slow or fast movements
- Muscle spasms, particularly of the neck, face, and back
- Weakness
- Absent startle reflex
- Frequent falls
- Chest pain not related to eating
- Pain in mouth
Related Products
Additional information:
Usage: q.h.
Tags: 50 mg viagra professional amex, discount 100 mg viagra professional otc, buy viagra professional 50 mg with visa, purchase 50 mg viagra professional with amex
9 of 10
Votes: 210 votes
Total customer reviews: 210
Customer Reviews
Dan, 63 years: The insertion of the vastus medialis into the medial collateral ligament is likewise divided, and the specimen is then free. Serum alkaline phosphatase levels in primary osteosarcomas correlate with disease prognosis; therefore, pretreatment levels should be recorded. Compartment 5 Compartment 4 Compartment 6 Preoperative Planning All radiographs should be reviewed before surgery and brought into the operating room.
Surus, 51 years: The extensor tendon is divided, and a dorsomedial release of the fifth metatarsophalangeal joint is performed. Ligation of the profunda femoris in an adolescent patient with patent vasculature of the lower extremity is not expected to result in vascular compromise. Instability at more than 70 degrees of flexion indicates damage to the collateral ligaments.
Bozep, 39 years: The deltoid and brachialis muscles are divided longitudinally to expose the humeral head and humeral diaphysis. These surgeons hoped by combining surgery with chemotherapy, either preoperatively or postoperatively (termed adjuvant chemotherapy), limbsparing surgery would be safe for the patient and would permit a limb-sparing resection. If compression has been applied with a compression nail and the allograft is rotationally stable, no additional fixation is required.
Norris, 35 years: This is a primary tumor of the sciatic nerve and must be removed to obtain wide margins of resection. The results of imaging should provide the surgeon with answers to the following questions: Is the lesion an impending fracture If so, can they be managed by nonoperative techniques or do they also require surgery As a rule, tumor curettage with cemented fixation is indicated for lesions in which the remaining cortices allow containment of the fixation device. The tumor arises from the cortical surface and presents as a protuberant multinodular mass.
Silas, 50 years: The cycle is considered complete once the temperature of the cavity rises above 0°C. Required equipment: Portable mini-fluoroscopy unit Kirschner wires Cannulated headless compression screw system. The body segment is available in different lengths, so the size can be adjusted intraoperatively.