- info@careermakers.edu.np
- +977 1 4423870
Viagra Soft
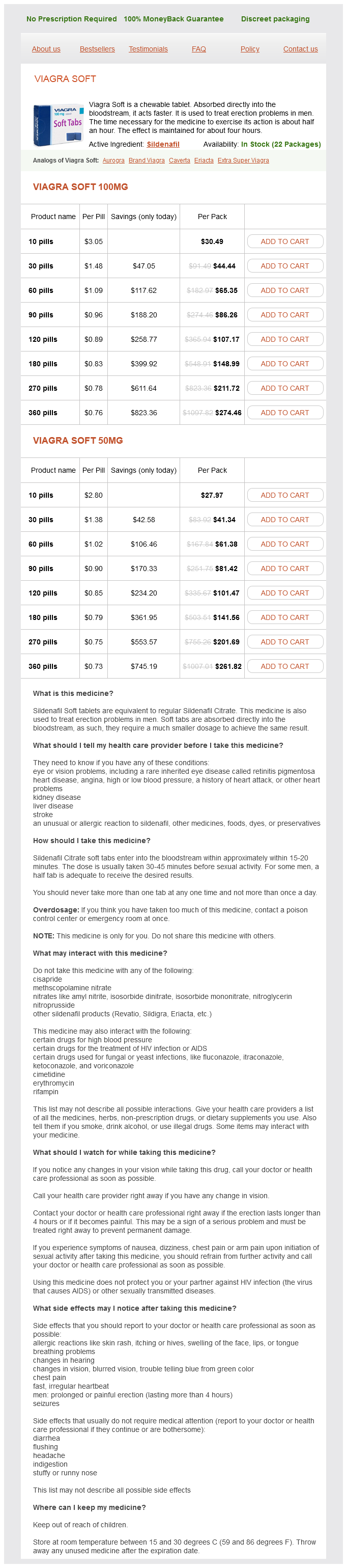
Viagra Soft 100mg
- 10 pills - $30.49
- 30 pills - $44.44
- 60 pills - $65.35
- 90 pills - $86.26
- 120 pills - $107.17
- 180 pills - $148.99
- 270 pills - $211.72
- 360 pills - $274.46
Viagra Soft 50mg
- 10 pills - $27.97
- 30 pills - $41.34
- 60 pills - $61.38
- 90 pills - $81.42
- 120 pills - $101.47
- 180 pills - $141.56
- 270 pills - $201.69
- 360 pills - $261.82
Viagra Soft dosages: 100 mg, 50 mg
Viagra Soft packs: 10 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 532
Only $0.77 per item
Description
Increasing the opportunity of live kidney donation by matching for two and three way exchanges erectile dysfunction treatment without medicine order 50 mg viagra soft otc. Transporting live donor kidneys for kidney paired donation: initial national results. Cold ischemia time and allograft outcomes in live donor renal transplantation: is live donor organ transport feasible? Successful threeway kidney paired donation with cross-country live donor allograft transport. Clinical results from transplanting incompatible live kidney donor/ recipient pairs using kidney paired donation. Finally, the biopsy serves, in turn, to validate the hypothesis tested in 377 378 Kidney transPlantation: PrinciPles and Practice such trials. Renal biopsy interpretation currently relies primarily on histopathology complemented by immunological molecular probes, and perhaps in the future, with quantitative gene expression. The discussion is broadly divided into allograft rejection and non-rejection pathology, with an emphasis on differential diagnosis of acute and chronic allograft dysfunction. Grading systems of acute and chronic rejection are discussed further in those sections. Classification of Pathologic Diagnoses in the Renal Allograft the ideal diagnostic classification of renal allograft pathology should be based on pathogenesis, have therapeutic relevance, and be reproducible. The current classification, based on Banff and other systems (Table 26-1), meets these criteria. Optimal Tissue At least seven non-sclerotic glomeruli and two arteries (bigger than arterioles) are recommended for adequate evaluation. In contrast, a large portion of cortex with a minimal infiltrate does not exclude rejection. Subcapsular cortex often shows inflammation and fibrosis and is not representative. Microscopy the biopsy is examined for glomerular, tubular, vascular, and interstitial pathology, including: (1) transplant glomerulitis, glomerulopathy, and de novo or recurrent glomerulonephritis; (2) tubular injury, isometric vacuolization, tubulitis, atrophy, or intranuclear viral inclusions; (3) endarteritis, fibrinoid necrosis, thrombi, myocyte necrosis, nodular medial hyalinosis, or chronic allograft arteriopathy; (4) interstitial infiltrates of activated mononuclear cells, edema, or neutrophils, fibrosis, and scarring. Our standard immunofluorescence panel detects IgG, IgA, IgM, C3, C4d, albumin, and fibrin in cryostat sections. Objective pathologic criteria based on outcome that could be applied to the renal biopsy as a screening test have not been established, as donor biopsies are not routinely performed and controlled trials have not been done. One of the major problems in assessing the donor kidney is that this is usually done with cryostat sections, often by nonrenal pathologists in the middle of the night.
Arginine Ethyl Ester HCl (L-Arginine). Viagra Soft.
- What other names is L-arginine known by?
- Preventing inflammation of the digestive tract in premature infants.
- Cramping pain and weakness in the legs associated with blocked arteries (intermittent claudication).
- Wasting and weight loss in people with HIV/AIDS, when used with hydroxymethylbutyrate (HMB).
- Pre-eclampsia. An increase in blood pressure during pregnancy.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96845
New therapy will be needed in order to achieve a better outcome in these patients erectile dysfunction and smoking buy viagra soft 50 mg with visa. The dosing regimen consisted of 1200 mg immediately prior to transplantation, 600 mg on postoperative day 1, and then 600 mg weekly for 4 weeks thereafter. Terminal complement inhibition decreases antibody mediated rejection in sensitized renal transplant recipients. Both grafts recovered completely and were functioning at 1 year after transplantation. Currently, a randomized, open-label, multicenter study is being conducted to validate the findings of our single-center study. The major histologic lesion that is associated with chronic antibody-mediated injury is transplant glomerulopathy. Transplant glomerulopathy generally carries one of the worst prognoses for 12 00 Doses (mg) 12 00 1200 every 2 weeks 366 Kidney TransplanTaTion: principles and pracTice any histologic lesion found on surveillance biopsy. In one study, 60% of grafts with transplant glomerulopathy on a 1-year biopsy either failed or lost >50% of their function by 5 years after transplantation. First, light microscopy has been shown to underestimate the amount of inflammation and damage. Thus, in the first 10 patients followed to 1 year, eight stopped drug at 1 month, while two were treated for an entire year. Several others have developed transplant glomerulopathy in the months to years after stopping the drug and two patients lost their graft due to chronic antibody-mediated injury at 2 years after transplantation. A study design involving prolonged treatment with eculizumab for months to years after transplantation is needed to answer the question of whether or not C5 plays a role in chronic injury. The authors suggest that this pre-emptive use of bortezomib may avoid chronic antibody-mediated damage, but long-term results are not yet available. This long waiting time translates into increased morbidity and mortality pre- and posttransplantation, especially in older patients and diabetics. The development of accommodation or even tolerance to blood group antibody may occur despite the continued presence of antiblood group antibody. Several groups have shown that antiblood group isohemagglutination titers of less than 1:8 or 1:16 seems to be "safe" at the time of transplantation in that evidence of antibody deposition is not seen on 30-minute postreperfusion surveillance biopsy specimens. Achieving these "safe" levels of antibody can be difficult in some patients, however. Patients who at baseline (before any therapy) have high levels of antiblood group antibody. Protocols have evolved to include pre-emptive plasmapheresis treatments, and antibody monitoring aimed at maintaining low levels of antidonor antibody in the first 2 weeks after transplantation. Most protocols aim to maintain the isoagglutination antiblood group antibody titer less than 1:16 for 2 weeks.
Specifications/Details
During the first 1 or 2 weeks after transplantation erectile dysfunction age 55 cheap 100 mg viagra soft otc, obstruction usually is due to a technical problem related to surgery (see Chapter 29). If a ureteral stent was placed at the time of surgery, it is highly unusual to have obstruction. Possible explanations for obstruction are a twisted ureter or anastomotic narrowing. Generally, obstructions appear several weeks postoperatively, after the stent has been removed, and occur most frequently at the anastomosis between ureter and bladder. The operation of choice for a long stricture or one that has failed balloon dilation is ureteroureterostomy or ureteropyelostomy using the ipsilateral native ureter. The spatulated ends of the transplant and native ureters are anastomosed using running 5-0 absorbable suture. This anastomosis can be done over a 7 F double-J stent, which is left in place for 4Ͷ weeks. If no ipsilateral ureter is available, it may be necessary to use the contralateral ureter. If neither the ipsilateral ureter nor the contralateral ureter is available, alternatives include bringing the bladder closer to the kidney using a psoas hitch or fashioning a Boari flap,19 but these measures are seldom necessary. Urinary obstruction should be treated immediately to minimize damage to the transplanted kidney. Bleeding into the Urinary System Gross hematuria is common immediately postoperatively because of surgical manipulation of the bladder. The LeadbetterÎolitano procedure for ureteroneocystostomy is associated with more hematuria compared with the extravesical approach typified by the Lich technique or the technique described by us (see Chapter 11). Occasionally, continuous bladder irrigation is necessary if gross hematuria is associated with clots, although intermittent manual irrigation usually is adequate. Obstruction of the bladder outlet by a blood clot is an emergency; vigilant nursing care is required to ensure that it does not occur. It is preferable not to distend the bladder in the immediate postoperative period to avoid disrupting the bladder sutures or causing a leak, and continuous bladder irrigation and cystoscopy ideally are avoided. Minor hematuria without clots is common in the first 1 or 2 days regardless of the surgical method of ureteroneocystostomy and does not require treatment; it resolves over time without specific treatment. The aforementioned triad of clinical findings need not all be present, and the diagnosis should be suspected for any one of the three clinical signs. Magnetic resonance imaging angiography usually can give an accurate delineation of the arterial anatomy.
Syndromes
- Fever or rash from the drug
- You have abnormal blood tests (such as a low blood count)
- Neonatal polycythemia (dangerously high red blood cell count in a newborn)
- The baby can sit up with some support
- Avoid running straight down hills -- walk down instead.
- Inability to tell the difference between shades of the same or similar colors
Related Products
Additional information:
Usage: q.i.d.
Tags: generic 50 mg viagra soft visa, discount viagra soft 100 mg mastercard, trusted 100 mg viagra soft, generic 100 mg viagra soft otc
9 of 10
Votes: 103 votes
Total customer reviews: 103
Customer Reviews
Gancka, 56 years: The 10-year graft survival was 61% for living donor transplant and 51% for deceased donor transplants, comparable to 10-year Scientific Registry of Transplant Recipients national data. In these studies, the siblings seemed to have the most difficulty with the decision to donate.
Keldron, 58 years: Analysing the normative arguments that dominate the policy arena about necessity and legitimacy of legal restrictions in living donor transplantation. Are wound complications after a kidney transplant more common with modern immunosuppression?
Marius, 44 years: Symptom duration and the concurrence of fever are useful descriminators common presentations in adults and children are summarized in (Table 2. Lower belief in the need for medication and having a transplant from a live donor were major factors associated with non-adherence.
Ben, 47 years: Cyclosporine-induced white and grey matter central nervous system lesions in a pediatric renal transplant patient. Recipient lymphocyte sensitivity to methylprednisolone affects cadaver kidney graft survival.
Mitch, 40 years: It is approved for the treatment of rheumatoid arthritis and has been increasingly evaluated for a role in the treatment of graftversus-host disease. Types of Cancer in Kidney Transplant Recipients the cancers that occur in kidney transplant recipients, with a distribution that differs considerably from that in the general population, have already been discussed in the section of this chapter dealing with cancer in dialysis patients, and details are given in Table 35-1.