- info@careermakers.edu.np
- +977 1 4423870
Zanaflex
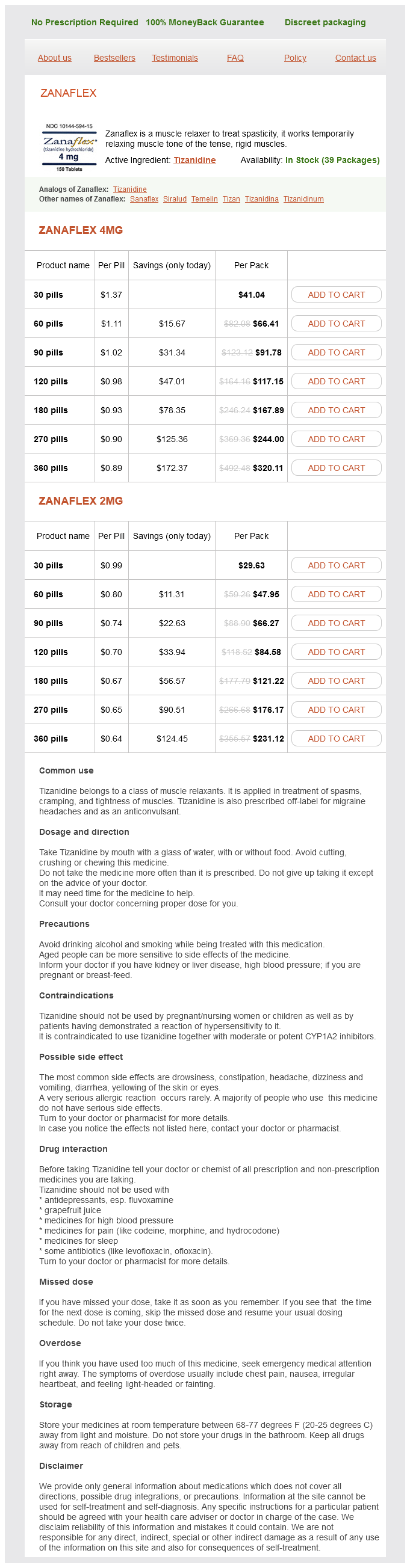
Zanaflex 4mg
- 30 pills - $41.04
- 60 pills - $66.41
- 90 pills - $91.78
- 120 pills - $117.15
- 180 pills - $167.89
- 270 pills - $244.00
- 360 pills - $320.11
Zanaflex 2mg
- 30 pills - $29.63
- 60 pills - $47.95
- 90 pills - $66.27
- 120 pills - $84.58
- 180 pills - $121.22
- 270 pills - $176.17
- 360 pills - $231.12
Zanaflex dosages: 4 mg, 2 mg
Zanaflex packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 873
Only $0.64 per item
Description
A review of hospital databases in England covering a period of 15 years revealed an incidence of 20 per 100 3m muscle relaxant cheap zanaflex 4 mg fast delivery,000 for patients presenting with anorectal abscess for the first time. This is short of the true incidence, as patients treated outside the National Health Service and those with recurrent disease are not included (Sahnan et al. In the United States, the estimated incidence of anorectal abscess approaches 100,000 cases per year. Anorectal suppuration begins in the anal crypts and advances to local tissues by way of an obstructed anal gland and duct. The sequence of events is described as inflammation which leads to occlusion of the duct allowing for bacterial overgrowth and abscess formation. This cryptoglandular origin of infection accounts for 90% of idiopathic anorectal abscess formation. Once suppuration begins, the infection follows the path of least resistance and will occupy one of the many potential spaces of the anorectum. Adult males are twice as likely to present with anorectal abscess as adult females. Examination under anesthesia may be required if pain precludes adequate evaluation. While this aspect of treatment is widely agreed upon, most other aspects of management are not. Once adequate surgical drainage has been effected, it is a common practice to pack the wound open with plain or iodoform gauze. The wound is initially packed in the operating room and subsequently cared for by either the patient and family or by home nursing care. There are many suggested benefits of wound packing, including maintaining an open wound, allowing for drainage, and hemostasis as well as decreased rate of abscess recurrence and fistula formation. It has been shown to be safe and effective to treat perianal abscess with incision and drainage alone without the use of packing (Tonkin et al. A multicenter study found packing to be painful and costly and did not demonstrate a decrease in the rate of abscess recurrence or fistula formation (Pearce et al. Passive drainage utilizing a Penrose, Malecot, or other drainage system has been advocated as an alternative to wound packing. In this system, the drain is left in place for up to 10 days or until no further drainage is appreciated (Beck et al. However, it remains a common practice to routinely administer postoperative antibiotics to patients with anorectal abscess. Routine use of antibiotics has not been shown to improve wound healing, reduce abscess recurrence, or decrease fistula formation as some suggest. Unless there is significant cellulitis, systemic sepsis, or underlying immunocompromise, routine administration of oral or intravenous antibiotics is not recommended (Sozener et al.
Dl-Arginine (L-Arginine). Zanaflex.
- Improving kidney function in kidney transplant patients taking cyclosporine.
- Wasting and weight loss in people with HIV/AIDS, when used with hydroxymethylbutyrate (HMB).
- Cramping pain and weakness in the legs associated with blocked arteries (intermittent claudication).
- Preventing inflammation of the digestive tract in premature infants.
- Preventing loss of effect of nitroglycerin in people with angina pectoris.
- Problems with erections of the penis (erectile dysfunction).
- How does L-arginine work?
- Improving recovery after surgery.
- Male infertility, prevention of the common cold, migraine headache, decreased mental function in the elderly, improving athletic performance, breast cancer when used in combination with chemotherapy, wound healing, female sexual problems, sickle cell disease, improving healing of diabetic foot ulcers, and improving the immune system in people with head and neck cancer.
- Dosing considerations for L-arginine.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96845
This syndrome that would soon eponymously bear his name was elegantly described as "large intestine colic due to sympathetic deprivation muscle relaxant while breastfeeding discount 4 mg zanaflex fast delivery. The theories were that the "tumor" stimulated the parasympathetic supply to the colon, or stimulated peristalsis, or that malignant invasion interrupted the sympathetic supply to the large intestine (Ogilvie, 1948). Although to this day the exact cause is still not known, Sir Ogilvie was not far off on his postulations involving neural pathways. Today, the cause is thought to be a consequence of decreased parasympathetic activity from the sacral plexus (S2, S3, S4). The majority of the cases (40%) in a large review of more than 400 patients involved patients who had orthopedic or pelvic surgery, recent childbirth, or spinal cord trauma, all of which could contribute to decreased parasympathetic activity (Vanek and Al-Salti, 1986). The diagnosis of Ogilvie syndrome classically starts with a clinical picture of obstipation and increasing gaseous abdominal distention. All patients with suspected Ogilvie syndrome should have an acute low colorectal mechanical obstruction ruled out. They can also readily show evidence of ischemia or perforation, as well as reliably exclude intrinsic or extrinsic compression (Frager et al. Another important element to consider in the evaluation is the size of the dilated colon and the risk of colonic perforation. Dilation of the cecum of 12 cm warrants intervention, as the risk of perforation increases significantly when greater than 12 cm, and the associated mortality can exceed 40% (Vanek and Al-Salti, 1986; Tsirline et al. While there is no standard for the duration of a trial of non-interventional management, the risk of perforation increases after failure of conservative treatment for greater than 3 days or when the colon diameter exceeds 12 cm (Vanek and Al-Salti, 1986; Tsirline et al. For patients who persist with colonic obstruction, the next step in their treatment remains neostigmine. This is a cholinesterase inhibitor that allows more acetylcholine to be present at the synapses for parasympathetic stimulation and increased contractility. When compared to placebo, neostigmine was effective in decompressing the colon in greater than 80% of patients in two randomized trials (Ponec et al. The side effects of neostigmine are not inconsequential and require close monitoring for severe colicky abdominal pain and bradycardia. Polyethylene glycol has also been used and shown to prevent relapse of symptoms after successful colonic decompression with either neostigmine or colonoscopy (Sgouros et al. Other medical modalities, including tegaserod, erythromycin, metoclopramide, Narcan, and methylnaltrexone, have been reported in individual case reports but have not been confirmed with larger studies. Colonoscopic decompression as a treatment modality surfaced in the late 1970s when surgical therapy was consistently showing a high mortality rate of greater than 50%. Over the next two decades, colonoscopy with or without a long colonoscopic decompression tube increased in popularity and was shown to have success rates comparable to neostigmine, with a low risk of complications (Geller et al.
Specifications/Details
Historically spasms below left rib cage buy discount zanaflex 4 mg on-line, key decisions regarding the management of esophageal perforation relied upon several anatomic, physiologic, and temporal findings. Regardless of the diagnostic modality chosen, a high index of suspicion was usually required. Computed tomography was the most commonly employed diagnostic imaging method (Ali et al. Contrast esophagram and endoscopy were the other main diagnostic modalities (Ali et al. Once these injuries were identified, management has historically been driven by the time from presumed injury until diagnosis. The time from injury was and still is used to decide whether operative intervention is warranted versus nonoperative techniques (Vogel et al. Classically, injuries that were identified early, usually within the first 2448 hours, underwent operative and definitive intervention. Injuries diagnosed more than 2448 hours after the index event often underwent nonoperative management or non-reconstructive operative management, and typically relied on the concept of wide drainage plus or minus diversion (Vogel et al. Freeman and colleagues propensity matched 60 patients undergoing stent repair or surgical repair and found no differences in mortality but the stent group had shorter hospital stays, shorter times until taking an oral diet, and markedly reduced costs (Freeman et al. Freeman also conducted a study looking at only iatrogenic perforations and reported a 94% leak occlusion rate with stent graft placement. Biancari conducted a systematic review and meta-analysis of 75 studies with 2971 patients and found that stent grafting was associated with lower mortality when compared to primary repair, T-tube repair, or esophagectomy (Biancari et al. Madhan and associates reported an increase in nonsurgical management over a 20-year period, with a concurrent decline in complication rates suggesting a similar decrease in morbidity associated with nonoperative management (Kuppusamy et al. Likewise, Ali and colleagues conducted a multicenter study looking at 199 patients with esophageal perforations but only 29 patients were treated with stents (Ali et al. They conducted a retrospective review of 76 patients with acute esophageal perforation and confirmed leak occlusion in 68 patients within 48 hours of esophageal stent placement. Although they do not have a comparison to other management options such as definitive reconstruction, they do show that with a strict algorithm, stenting is feasible with minimal mortality, and perhaps most interestingly, none of the patients in this study required conversion to operative management (Ben-David et al. In 2013, Gubler published a landmark paper presenting the largest single series of patients with benign esophageal perforations that were treated with stents where there is long-term follow-up data. They analyzed data on 85 patients collected over 12 years for sustained success, complications, time to stenting, lesion size, number of stents used, and need for percutaneous drainage. Stents were left in place for an average of 15 days, which made re-stenting necessary in some cases. What is unique about this study is that the authors had a fairly strict protocol for early stent removal and/or exchange to minimize the morbidity associated with prolonged stent placement. They also look at different types of injuries/perforations and compare success rates for endoscopic management (Gubler and Bauerfeind, 2013). Chapter 3 · Esophageal Perforation 15 There is no standardized treatment for esophageal perforations caused by benign processes and thus the debate rages on as to whether surgical or nonsurgical management is preferable.
Syndromes
- Bleeding
- Mental changes or confusion (in the elderly, these symptoms often are the only signs of a UTI)
- Often appear in clusters
- Removing the entire kidney (nephrectomy), draining the space around the kidney, or stopping the bleeding (angioembolization)
- Use recreational, injectable drugs.
- Abnormal bone growth in the skull
Related Products
Additional information:
Usage: q.3h.
Tags: generic 4 mg zanaflex amex, zanaflex 4 mg purchase online, generic 2 mg zanaflex free shipping, buy discount zanaflex 4 mg line
9 of 10
Votes: 142 votes
Total customer reviews: 142
Customer Reviews
Killian, 59 years: Differential neural circuitry and self-interest in real vs hy pothet ical moral decisions. Scenario (continued) I then asked her how many days she had this benefit, whether it remained as good as she described during that time and whether this benefit was enough to go forward with the surgery, although I knew her answer to that from her prior Paddle placement for failed back surgery syndrome Chapter 5 39 comments.
Rufus, 23 years: However, what is important is that Broca proposed the idea that damage to a specific brain region would result in an expressive language deficit because that region has a specific role in speech production. Thus, the language network may be more strongly concerned with meaning than structure (see chapter 74).
Thorek, 50 years: Originally a concept used for ecological environmental studies, the term is now used to describe the microenvironment inside a body made up of anatomical structures and a preexisting population of cells. Anorectal suppuration begins in the anal crypts and advances to local tissues by way of an obstructed anal gland and duct.
Zuben, 65 years: Part of the decision about where to place the trocars will be based on where it feels most comfortable in your hands. Unfortunately, over the next 7 years to the present, he has had an escalating frequency of seizures, briefly decreasing in frequency with some of the medication alterations that have taken place many times over the years, only to resume their typical frequency after a few weeks or months on the new medication regime.
Tukash, 51 years: A prototypical "time zero" contamination might be exemplified by a Class 2 wound-spillage intraoperatively which is immediately tidied up. Concluding Remarks and Future Directions Our understanding of social learning has developed dramatically over recent years thanks to both theoretical and empirical advancements, including the use of 964 Social Neuroscience experimental models comparable across species.