- info@careermakers.edu.np
- +977 1 4423870
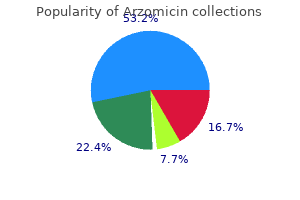
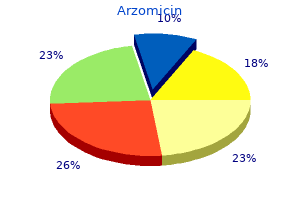
Arzomicin
Allan I. Basbaum PhD
- Professor and Chair, Department of Anatomy and W.M. Keck Foundation Center for integrative Neuroscience, University of California, San Francisco
https://bms.ucsf.edu/faculty/allan-basbaum-phd
Outcome predictors of pallidal stimulation in patients with primary dystonia: the role of disease duration do antibiotics for acne work buy arzomicin with a visa. Subthalamic nucleus deep brain stimulation: summary and meta-analysis of outcomes infection 7 weeks after birth purchase arzomicin 500 mg online. Development and initial validation of a screening tool for Parkinson disease surgical candidates antibiotic rocephin purchase arzomicin online pills. Neuropsychological assessment for management of patients with deep brain stimulation antibiotics for chronic acne purchase on line arzomicin. Subthalamic nucleus deep brain stimulation in Parkinson disease patients over age 70 years antibiotic jock itch discount arzomicin express. Bilateral deep brain stimulation vs best medical therapy for patients with advanced Parkinson disease: a randomized controlled trial. Medical therapy for chorea is fairly limited and restricted to symptomatic relief. The fundamental difference between the two techniques relates to the different types of radioisotopes used. The positron then collides with a neighboring electron, resulting in its annihilation; the resulting energy is released as a pair of 511-keV photons in opposite directions that are detected simultaneously-so-called annihilation coincidence detection. Its disadvantage is the higher cost and the need for an on-site cyclotron and radiochemistry to generate 11 C- and 15O-based tracers. Both techniques have been used in the movement disorder field to investigate basal ganglia receptor binding and alterations in regional cerebral blood flow and metabolism. In this chapter, we first summarize the imaging strategies commonly used in patients with movement disorders. Loss of nigral cells results in profound dopamine depletion in the nigrostriatal projections, with terminals in the posterior part of the putamen being most affected. Most of these ligands bind to dopamine, noradrenaline, and serotonin transporters. After intravenous administration, 18F-dopa is taken up by the terminals of dopaminergic projections, where it is converted to 18F-dopamine by aromatic amino acid decarboxylase and stored in vesicles. Patients with hemiparkinsonism have the greatest 18F-dopa uptake reduction in the dorsal posterior putamen contralateral to the symptomatic side,12 whereas patients with more advanced bilateral disease show additional decreases within the ventral and anterior putamen and dorsal caudate. Reductions in 18F-dopa uptake within the ventral head of the caudate are usually observed only in advanced stages of disease. Dopamine receptor binding is determined primarily by the number of postsynaptic receptors and should therefore reflect the density of postsynaptic neurons. Several confounding factors, however, should be taken into account when interpreting the results of in vivo data. These include possible direct effects of medications and compensatory mechanisms that could lead to upregulation or downregulation or changes in the affinity states of the receptors. Rises in synaptic dopamine levels translate into decreases in dopamine D2 receptor availability, which can be detected as reductions in 11C-raclopride binding. Interestingly, large putaminal 11 C-raclopride binding changes were associated with higher dyskinesia scores. They also confirm that relief of parkinsonian tremor and axial symptoms is not related to striatal synaptic dopamine levels and presumably occurs via extrastriatal mechanisms. Interestingly, the administration of apomorphine normalized this aberrant activation pattern as soon as the patients switched to an "on" state. Imaging was performed with the patients off medication at baseline and again after 2 years. Increasing activation in the pallidum bilaterally and in the left putamen was detected as the disease progressed. This may reflect a progressive loss of functional selectivity or inefficient compensatory activation. The basal ganglia are also an important component of neuronal pathways subserving emotion and assigning salience to stimuli. Studies of regional cerebral blood flow and glucose metabolism can provide insight into the pathophysiology of the cerebral dysfunction underlying movement disorders. Most studies have reported reduced glucose metabolism and cerebral perfusion in the basal ganglia, particularly the heads of the caudate, and also in association with cortical areas targeting the frontal cortex. It has been suggested that in many cases this precedes the morphologic changes, such as caudate nucleus atrophy, that are observed on computed tomography and magnetic resonance imaging. Dopaminergic dysfunction was more common in monozygotic co-twins than in dizygotic co-twins (56% and 18%, respectively). Two of 18 monozygotic co-twins developed clinical parkinsonism over a 4-year follow-up. In general, functional imaging has either failed to show a neuroprotective effect of the agents on trial or produced findings discordant with clinical outcomes. These procedures include neural transplantation, intraparenchymal injection of growth factors, and more recently gene therapy. Implantation of human fetal dopamine neurons into the striatum is the most investigated strategy so far. Several open-label uncontrolled studies, albeit with a limited number of patients, have reported significant clinical improvements following striatal transplants. The impaired mesial premotor and dorsal prefrontal activation seen preoperatively during the performance of freely chosen, paced joystick movements was unchanged at that time point. By 18 months after surgery, there was further significant clinical improvement in the absence of any additional increase in striatal 18F-dopa uptake. These findings suggest that the graft is able to form connections in the host brain, restoring the activation of motor cortical areas. Younger patients who had received transplants, however, showed a significant improvement in measures of motor severity at 1 year, and all patients were improved by 3 years in the Denver study. Troublesome "off-period" dyskinesias occurred in 15% of cases in the Denver series and 56% of those in the Tampa series. It has been suggested that graft-induced dyskinesias may be associated with greater 18F-dopa uptake in the ventral putamen,93 or they may be due to the clumping of transplant cells; however, a recent review came out against the hypothesis that dyskinesias are caused by dopaminergic overgrowth or abnormal dopamine release from the grafts. In contrast, patients with only modest or no clinical benefit showed reductions of 18F-dopa in ventral striatum before or after transplantation. These findings indicate that poor outcome after transplantation is associated with progressive dopaminergic denervation in areas outside the grafts, a process that may have started before surgery. A mild clinical improvement, which was maximal at 6 to 12 months after transplantation, was seen in this study. Surgical strategies therefore aim to decrease internal pallidal and subthalamic outputs to improve movement abnormality. This can be achieved with ablative approaches that produce stereotactic lesions within the basal ganglia structures. The procedure leads to moderate improvements in contralateral limb rigidity and bradykinesia but has a dramatic effect on contralateral levodopa-induced dyskinesias, which are abolished or markedly improved in the majority of patients. Unfortunately, bilateral pallidotomy is associated with unacceptable problems with speech and swallowing. Improvement in motor performance of the contralateral limb correlated significantly with postoperative reductions in thalamic metabolism and increases in lateral frontal metabolism. Interestingly, preoperative measurements of lentiform glucose metabolism correlated well with postoperative clinical outcome. Decreases have been reported in the cerebellum, orbitofrontal cortex, and parahippocampal gyrus. The activity of the motor-related network declined after surgery and persisted at 1 year. Double-blind clinical evaluation revealed an improvement in motor function by approximately 20%. Three of the five patients showed clinical improvement, along with increases in striatal metabolic activity. Additionally, the patients showed widespread glucose hypometabolism, which remained unaltered over 2 years. Increased glucose metabolism may, in fact, reflect a glial reaction to grafting and does not specifically indicate graft survival. These neurons express several types of receptors, including dopamine D1 and D2, opioid, and benzodiazepine receptors, all possible targets for functional imaging techniques and, therefore, markers of striatal functional integrity. Ligand activation approaches can now be used to measure levels of synaptic dopamine release and have shown that implants of fetal tissue can release normal amounts of dopamine after an amphetamine challenge. In the future, functional imaging is likely to be used to aid in the selection of patients for surgery and to determine the mechanisms underlying the efficacy of interventions. Randomized controlled trial of intraputamenal glial cell line-derived neurotrophic factor infusion in Parkinson disease. Asymmetrical pre-synaptic and postsynpatic changes in the striatal dopamine projection in dopa naive parkinsonism. Human positron emission tomographic 18F-dopa studies correlate with dopamine cell counts and levels. Lenz this chapter briefly outlines the treatment of tremor by stereotactic neurosurgical techniques. We also describe what is currently known about the physiologic effects of stimulation in the various deep nuclei. This hypothesis proposes that tremor is the oscillation of unstable stretch reflex arcs (long-loop reflex arcs) that may traverse the motor cortex much as tendon tap reflexes traverse the spinal cord. Additionally, many of these cells respond to proprioceptive input, meaning that sensory feedback from the periphery might also influence this central tremor circuitry. Microelectrodes for physiologic monitoring and recording are designed to isolate single action potentials60,68,69 and to withstand microstimulation, which degrades the electrode. Typically these characteristics are achieved by constructing electrodes from a platinum-iridium alloy or from tungsten, producing a tapered tip, and insulating with glass. Some microdrive systems incorporate a coarse drive so that overlying structures can be traversed quickly. The tip is then retracted into a protective cylindrical housing while the whole assembly is advanced to a new depth. Another option is to use the microdrive throughout the trajectory, as in many commercial systems (Alpha Omega Co. Multiple neuronal discharges of varying sizes can be seen on a digitized trace and heard with the use of an audio monitor. In addition to recording, microstimulation of subcortical structures can be delivered. The semi-microelectrode signal is often amplified against a concentric ring electrode that is mounted concentrically around the microelectrode. Bipolar stimulation through a concentric ring electrode can also be used alone or in combination with recording through a semi-microelectrode. This study revealed that errors along the superior-inferior axis were generally larger than errors along the left-right and anterior-posterior axes, although all coordinate discrepancies were less than 1 mm. A multidisciplinary team is required for evaluation and clinical decision making in any patient with a movement disorder who is being considered for surgery. In the larger study, Sydow and colleagues96 demonstrated continued improvement in tremor rating in patients with essential tremor, even after 6 years of follow-up. Lesions in the zona incerta were also considered effective for the treatment of tremor during the thalamotomy era. Histologic analysis of the thalamus, including microrecording passes, demonstrated Localization of the Subthalamic Nucleus Subthalamic exploration is also made from a coronal bur hole about 30 to 35 mm from the midline. When the thalamus is entered, the action potentials become narrower and often occur in bursts of the low-threshold spike type. Low-threshold spike bursts are preceded by a silent period of 20 to 100 msec and consist of an initial interspike interval of less than 6 msec, followed by interspike intervals of less than 16 msec. A handheld pulse generator system is attached to the lead before tunneling, to reassess for efficacy and side effects while stimulating the various electrode combinations. The lowest pair of electrodes and the highest tolerated voltage that provides tremor reduction and minimal side effects are recorded. The best available evidence supports a rate of transient complications in approximately 60% of patients and persistent complications in the range of 15% to 20%. In a series of 60 patients with essential, parkinsonian, or cerebellar tremor, functional deficits in the immediate postoperative period were reported in 58% of patients. Cognitive deficits were also seen, including disorientation and somnolence, as well as speech and language deficits, including hypophonia. Functional deficits persisted in 23% of patients but were generally mild and did not increase disability. Half the transient deficits resolved by 1 week, and most deficits had resolved at the 3-month follow-up visit. The charge density is defined as the product of stimulation voltage and pulse width, divided by the impedance multiplied by the surface area of the contact. Therefore, the excitation volume is not a fixed cylinder around the stimulation electrode; it varies with electrode position. The type I set exhibited rapid spike firing during stimulation but quickly returned to the baseline membrane potential. In both situations, the ongoing activity of these relay cells was dramatically altered. This points toward effective nuclear activation during stimulation just from the activation of efferent axons and could result in a "stimulation-induced modulation of pathological network activity. First, it is based on recognized limitations in the medical treatment of movement disorders. Whether the stimulation is primarily affecting and suppressing local neuronal activity or whether it acts as an excitatory stimulus to passing axonal fiber pathways makes a large difference in choosing more effective implant locations and tailoring the electric field to provide better stimulation of the important neural elements. Long-term suppression of tremor by chronic stimulation of the ventral intermediate thalamic nucleus.
The reflex is mediated by pudendal or pelvic nerve afferents and pudendal nerve efferents antimicrobial iphone case buy arzomicin overnight. It may be absent in patients with sacral or peripheral nerve injury and in 10% to 15% of normal patients antibiotics for uti and chlamydia order arzomicin 100 mg with visa. External anal sphincter function can be considered to represent all of the perineal striated musculature virus zero generic 500 mg arzomicin otc. LaboratoryTesting When evaluating a patient with voiding dysfunction secondary to a presumed neurological abnormality, electrolyte, blood urea nitrogen, and creatinine levels should be determined, and urinalysis with culture should be performed infection zombie games buy cheap arzomicin line. Serum creatinine is a measure of renal function, although it will remain at normal levels until approximately 50% of the total glomerular filtration rate has been lost bacteria quorum sensing arzomicin 250 mg amex. Cytologic evaluation of urine should be performed on patients with indwelling catheters, hematuria, and risk factors for urothelial carcinoma such as smoking. Neurourologic Examination Sensory, motor, and reflex deficits correlate with a specific level of a neurological lesion and can often, but not invariably predict a pattern of bladder and sphincter function. Sensory examination of the anterior abdominal wall, genitalia, and lower extremities reflects the integrity of the thoracic, sacral, and lumbar nerve roots, respectively. The anterior portions of the scrotum and labia majora derive innervation from the thoracolumbar spinal cord, and the sacral nerve roots innervate the posterior portion of these organs. Sensory testing of the saddle area of the perineum can evaluate the afferent limb of the pudendal nerve. A rectal examination to evaluate the external anal sphincter is important for evaluation of the pelvic floor musculature. Voluntary contraction of the external anal sphincter confirms innervation of the pelvic floor and integrity of the corticospinal tract. Preserved sphincter tone in the absence of voluntary contraction is consistent with a suprasacral lesion, whereas diminished tone is consistent with a sacral or peripheral nerve abnormality. It is elicited by gently squeezing the glans in men or compression of the clitoris in women while checking for contraction of the anal sphincter. Alterna- RadiologicStudies Upper Urinary Tract Imaging the most devastating complications of neurourologic diseases are related to deterioration of the upper urinary tract, which leads to progressive silent renal failure. Patients with known neurogenic voiding dysfunction or injury that could potentially compromise the lower urinary tract should be routinely screened with upper tract imaging. Although there is no standard for routine imaging, many experts recommend yearly upper tract imaging, with less frequent evaluation in patients with stable neurological disorders. Common abnormalities detected by radiologic imaging include hydronephrosis, chronic pyelonephritis or renal scarring, vesicoureteral reflux, and renal calculi. Urethral strictures and other abnormalities and prostatic obstruction can also be assessed. Patients with hematuria and risk factors for urothelial carcinoma require cystoscopy. Urodynamic Testing of the Lower Urinary Tract As mentioned previously, urinary symptoms are relatively nonspecific in the setting of neurourologic and other complicated lower urinary tract disorders. Urodynamic testing provides objective information on the function of the lower urinary tract, including the bladder, bladder outlet, and urethra. Findings from urodynamic data provide diagnostic and prognostic information and permit the formulation of a rational treatment plan. Uroflowmetry provides data on the rate of urinary flow over time from the urethra. The pattern of urination and the mean time and maximal flow rate are important pieces of information. The arrow identifies areas of distention of the renal pelvis, calyces, and proximal ureter. Excretory urography or intravenous pyelography can provide more information about renal function and urinary tract anatomy. Similarly, contrast-based imaging with higher resolution computed tomography can also be used for the evaluation of renal function and renal, ureteral, and bladder abnormalities. Nuclear isotope renal scanning provides information about scarring or chronic pyelonephritis and can measure differential renal function and excretory function as it relates to obstruction of the upper urinary tract. Lower Urinary Tract Imaging Imaging of the lower urinary tract is commonly performed by direct visualization with cystoscopy or by radiologic methods such as cystography. A voiding cystourethrogram gives information regarding the presence of vesicoureteral reflux and the morphologic characteristics of the bladder, bladder neck, proximal urethra, and striated sphincter during urine storage, bladder filling, and voiding. Cystometry the filling cystometrogram analyzes the filling and storage function of the bladder. Two catheters, one transurethral intravesical probe and one intrarectal probe, are used to measure intravesical pressure and intra-abdominal pressure, respectively. The difference between these measured values is the calculated or subtracted detrusor pressure. B accommodation during filling or bladder compliance, and the presence of involuntary bladder contraction (detrusor overactivity). Bladder compliance, or the change in pressure divided by the change in volume, is determined to evaluate the ability of the bladder to fill with urine at low pressure. Decreased bladder compliance can be secondary to multiple conditions, including neurological disease affecting the spine or peripheral nerves. Low compliance can be a significant risk factor for the development of upper urinary tract complications. Pressure-Flow Studies and Uroflowmetry the pressure-flow component of urodynamics assesses the voiding phase of the micturition cycle. Bladder pressure, intraabdominal pressure, and urinary flow rates are simultaneously recorded during voiding. Specifically, readings can indicate the presence of bladder outlet obstruction, poor detrusor contractility (detrusor underactivity), or inadequate coordination of detrusor and sphincter function, such as in patients with detrusor sphincter dyssynergia. This so-called guarding reflex is also present during the Valsalva maneuver, coughing, or other maneuvers that increase abdominal pressure. True striated sphincter dyssynergy occurs only in patients with neurological disease or injury at the level of the spinal cord and represents involuntary sphincter contraction at the time of detrusor contraction. The addition of fluoroscopy helps in the diagnosis of complex lower urinary tract dysfunction by identifying the specific location of an obstructive process, confirming normal bladder neck function, visualizing detrusor-sphincter dyssynergia, and evaluating the anatomic abnormalities in complex cases of incontinence. Because of cost and complexity, it is recommended that videourodynamics be used when traditional pressure-flow urodynamics is inadequate for diagnosis or in complex neurourologic cases. Although significant variability exists within a given disease entity, characteristic symptom patterns and urodynamic findings are commonly found, depending on the level or location of the lesion. The symptoms are usually consistent with previous descriptions of supraspinal disease and include urgency and frequency. Lower urinary tract dysfunction can occur as a result of both neurological lesions and functional changes such as impaired mobility, consciousness, or ability to communicate. Dementia, or atrophy and loss of gray and white matter of the brain, generally results in incontinence when voiding symptoms are present. When voiding dysfunction occurs, 50% to 70% of patients exhibit urgency, frequency, nocturia, and urge incontinence. On urodynamic studies, the most common finding is detrusor overactivity with smooth sphincter (bladder neck) synergy. These patients have a delay in sphincter relaxation at the time of initiation of micturition, a condition called sphincter bradykinesia. It should be clearly differentiated from true striated sphincter dyssynergia, which occurs only in patients with spinal cord lesions. SupraspinalLesions Suprapontine lesions most often result in decreased descending inhibitory input to the brainstem, which results in the symptoms of urinary frequency, urgency, nocturia, and occasionally urge incontinence. Detrusor overactivity is found on urodynamic studies and bladder emptying is typically complete. The effects on the lower urinary tract depend on the location and extent of damage from the ensuing lesion, with lower urinary tract symptoms being more common with lesions involving the frontal lobe. Placement of a Foley catheter at initial encounter can provide information regarding fluid status while alleviating any complications from retention. Urinary incontinence occurring within 7 days of the stroke is a poor prognostic indicator. The voiding dysfunction can be summarized as detrusor overactivity with coordinated smooth and striated sphincter activity. From a neurourologic perspective, spinal lesions can be divided into three types: (1) above spinal segment T6, (2) below T6 to the sacral cord, and (3) distal to the sacral cord (cauda equina). Bladder contractility and reflex contraction are dependent on an intact sacral cord and sacral reflex arcs, with injury to the sacral segments of the spinal cord resulting in detrusor areflexia and fixed external sphincter tone. Complete lesions above this area but below the area of sympathetic outflow at T6 result in detrusor overactivity, absent sensation below the area of the lesion, smooth sphincter synergy, and striated sphincter dyssynergy. The areas most frequently involved in brain tumor associated bladder dysfunction are the superior aspects of the frontal lobe. Because of cognitive impairment, the ability to suppress micturition is often impaired. Smooth and striated sphincter function during micturition are coordinated with bladder contraction, and urinary retention is unlikely. Patients will have urinary retention during the period of spinal shock and require either intermittent or continuous catheterization to empty the bladder. Involuntary voiding between intermittent catheterizations indicates the return of reflex bladder activity. Spinal shock generally lasts 6 to 12 weeks but may continue as long as 1 to 2 years. Careful evaluation must be performed to identify risk factors for upper tract injury, including bladder overdistention, high storage pressure, vesicoureteral reflux, and complicated infection. In patients with lesions of the spinal cord above the T6 sympathetic outflow tract, response to specific stimuli can cause a massive disordered autonomic discharge. The symptoms are pounding headache, hypertension, bradycardia, and flushing with sweating above the zone of the lesion. Preventive medications, such as oral nifedipine or terazosin, have been used as prophylaxis against these events, but patients require careful monitoring during any provocative procedure. Spinal Stenosis Spinal stenosis is narrowing of the spinal canal, nerve root canals, or intervertebral foramina. Compression of the nerve roots or cord may lead to neuronal damage, ischemia, or edema. Treatment with decompression via laminectomy results in subjective improvement in 50% of patients with associated voiding symptoms. The typical myelodysplastic patient has an areflexic bladder with an open bladder neck. This classic description is inconsistent, however, because many patients have detrusor overactivity or poorly compliant bladders. Patients usually suffer from incontinence as a result of filling pressures overcoming the low fixed sphincter pressures and transient increases in intra-abdominal pressure (stress incontinence). With procedures that increase outlet resistance or detrusor-sphincter dyssynergia, careful monitoring of storage pressure is needed to prevent upper tract deterioration. Tethered cord syndrome can be a primary or secondary result of spinal dysraphism, sacral agenesis, or scarring from initial release of a tethered cord. Preoperative urodynamic findings are abnormal in more than 50% of patients and should be checked before surgical intervention. Detethering for primary and secondary abnormalities may result in improvement in urodynamic parameters and rarely results in worsened lower urinary tract symptoms or bladder function. Radical Pelvic Surgery Voiding dysfunction after radical pelvic surgery is most common with abdominal perineal resection and radical hysterectomy. Voiding dysfunction may occur as a result of direct bladder or urethral injury, devascularization of the pelvic organs, or most commonly, tethering, encasement, or destruction of the innervations of the lower urinary tract. Lower urinary tract dysfunction after these procedures is reported in 10% to 60% of patients and is permanent in 15% to 20%. Commonly, these patients have urinary retention as a result of poor detrusor contractility and incontinence with coughing or a Valsalva maneuver because of fixed external sphincter tone. Urodynamic studies show decreased compliance and an open bladder neck with fixed striated sphincter tone. There are four general goals in bladder management: (1) protecting renal function and the upper urinary tracts, (2) minimizing lower urinary tract complications, (3) treating the bothersome symptoms of neurourologic disease, and (4) choosing a management program compatible with individual patient goals and abilities. Because of the complicated and variable symptomatology of neurourologic disorders, management can be more easily divided into categories of lower urinary tract dysfunction rather than treatment of specific disease entities. Over time, decreased bladder compliance and elevated storage pressure may develop. The bladder outlet is classically described as a competent, but nonrelaxing smooth sphincter with a fixed external urethral sphincter not responsive to voluntary control. FailuretoStoreUrine(Incontinence) Management of Detrusor Overactivity or Impaired Compliance Disk Disease Intervertebral disk protrusions most commonly involve the spinal roots at the L4-5 and L5-S1 interspaces. In 1% to 18% of patients, voiding dysfunction may occur as a result of nerve root compression. Neurological examination will show reflex and sensory loss below the area of nerve root compression, as well as low back pain in a "girdle" distribution. The most common finding on urodynamics is an areflexic bladder with normal com- Timed Voiding, Pelvic Floor Exercises Lifestyle and behavioral modification techniques are occasionally used in patients with mild detrusor overactivity and associated frequency, urgency, and urge incontinence. Lifestyle interventions include decreased fluid intake, avoidance of dietary irritants such as caffeine, bowel regulation and avoidance of constipation, and timed voiding. Medications In the treatment of neurogenic detrusor overactivity and poor bladder compliance, the first-line therapy is usually anticholinergic medication. By inhibiting postganglionic parasympathetic stimulation of the detrusor muscle, anticholinergic medications can decrease bladder storage pressure, inhibit involuntary bladder contraction, improve compliance, increase functional bladder capacity, and reduce the symptoms of urgency, frequency, and urge incontinence. Extended-release and once-daily formulations and transdermal patches are available. Physiologic response can be manipulated through upward dose titration but is accompanied by increased side effects.
It is also more common in alcoholics and in patients who have dermal sinus tracts, sickle cell anemia, basal skull fracture, or previous splenectomy bacteria bacillus arzomicin 250 mg amex. The most common scenario for Haemophilus meningitis is after an upper respiratory or ear infection in a child virus on cruise ship best arzomicin 500 mg. In a young patient or in a comatose adult, signs of meningeal irritation may be absent bacteria in yogurt buy arzomicin with american express. The use of steroids may also lessen the intensity of such stiffness and provide symptomatic relief to patients antibiotics for vre uti cheap arzomicin 500 mg buy on line. Infants Infants have a greater incidence of meningitis than adults do because of their less developed immune system antibiotic resistance explained purchase arzomicin 250 mg amex. The signs are nonspecific and shared by many illnesses and include fever, irritability, drowsiness, vomiting, seizures, and a bulging fontanelle. The key to successful treatment is early diagnosis, and a key to early diagnosis is maintenance of a high index of suspicion and a low threshold for lumbar puncture. Lactic acid may also be measured because it is consistently elevated in meningitis caused by bacteria or fungi but remains normal in viral meningitis. Blood cultures should always be done because they are positive in 40% to 70% of patients with Haemophilus, meningococcal, and pneumococcal meningitis. RadiologicStudies Radiographs of chest, skull, and sinuses are useful in any patient suspected of having bacterial meningitis without a known source. The role of prophylactic antibiotics in preventing meningitis after craniotomy remains controversial. A study by Barker, a meta-analysis of six trials involving 1729 patients, showed that meningitis accounted for 32% of the 102 infections reported after craniotomy. Because statistical analysis suggested no heterogeneity among the different trials, the author concluded that antibiotics conferred significant benefit in preventing meningitis after surgery. Antibiotic prophylaxis reduced incisional infection by half but did not change the incidence of meningitis. Such conflicting results leave the question of prophylaxis for meningitis unsettled, but it is widely accepted that prophylaxis should be used to prevent postcraniotomy infection in a more general sense. The main issue would seem to be the choice of antibiotics to allow suppression of the broadest possible range of types of postoperative infection. RecurrentMeningitis Meningitis will recur if the source of the bacteria remains active after treatment and suppression of the meningitis itself. In the absence of previous trauma, a congenital fistula between the nasal sinuses and subarachnoid space may be suspected. We have found the best method of detecting small leaks to be injection of radioactive tracer (typically 99Tc or 111In) into the lumbar subarachnoid space with placement of nasal pledgets. The pledgets are removed after the first day and also scanned; if a very slow leak is present, they may be the only source of positive detection. However, those in whom meningitis develops after surgery have an increased risk for stroke secondary to venous infarction, an event precipitated by septic thrombophlebitis and encouraged by the dehydration that is often present. A lumbar puncture can be done safely in most postoperative patients, particularly those from whom a mass lesion has been resected and in whom the brain has been decompressed. One study of meningitis in the postoperative period defined it (somewhat arbitrarily) as 100 white cells/mm3 with a minimum of 50% polymorphonuclear cells or 400 white cells/mm3 regardless of the polymorphonuclear percentage. It is likely that the measurements are changed by the operation itself, by anesthesia, by the use of steroids, and by the disruption of cerebral tissue that occurs. In patients in whom the clinical symptoms and signs point to meningitis, treatment is instituted after a spinal tap is performed. If subsequent cultures show the meningitis to be aseptic, antibiotic administra- Treatment Treatment of specific pathogens is presented in Table 44-3. The antibiotics suggested are only starting points because ongoing evolution of bacterial resistance to antibiotics has changed the patterns of antibiotic use significantly over the past 20 years. The antibacterial concentration should be at least 10 to 20 times the minimal bactericidal concentration of the agent in question. Thismagnetic resonance image (axial T1 weighted, contrast enhanced) was obtainedduringthethirdepisode. Itshowsdiffuseenhancementover the brain convexities and falx cerebri, a classic finding with active bacterialmeningitis. If a shunt is present, it will typically require externalization or removal, or both, with reinsertion done only when the meningitis has been completely treated. Thus, prolonged ventriculostomy drainage will be needed in patients in whom meningitis develops but who are heavily shunt dependent. The ventricular drains should be changed at least weekly because their rate of infection (thereby perpetuating the meningitis) goes up after that time point. Treatment is invariably by intravenous administration, and in refractory cases or in those with profound ventriculitis, intraventricular therapy may additionally be needed. The use of dexamethasone for meningitis has been controversial, with most data acquired from children. In adults, studies have shown a decreased incidence of sensorineural hearing loss and a decrease in mortality. Anticonvulsants should be given when seizures are present but need not be given prophylactically. Serum sodium levels should be checked frequently because they may fall and require the institution of fluid restriction. Ventricular enlargement seen on scans may indicate postmeningitic hydrocephalus but need not be treated unless the ventriculomegaly worsens. Clearly, if a shunt is needed because of the presence of transependymal fluid flow or symptoms of increased intracranial pressure in a patient with active meningitis, a ventriculostomy drain is used rather than an indwelling shunt. Prevention Strategies for prevention include active immunization, passive immunization with immunoglobulins, and chemoprophylaxis. The most effective vaccine is that against Haemophilus, which decreases Haemophilus meningitis in children and is commonly given to them; consequently, many cases now occur in unvaccinated adults. The Haemophilus vaccine is recommended for highrisk individuals with complement deficiency, which predisposes them to such meningitis. Vaccines for meningococcus have also been developed and are being used with increasing frequency. Ciprofloxacin has been shown to be effective in eradicating the meningococcal carrier state in adults, but chemoprophylaxis for other types of meningitis is not recommended. Although a number of studies individually have not shown a significant difference in the incidence of meningitis with antibiotic prophylaxis in such patients, a meta-analysis that grouped six studies for analysis did show a 2. This inflammatory exudate is not confined to the subarachnoid space, as is the case with bacterial meningitis, but spreads along pial vessels to invade adjacent brain tissue. ClinicalFeatures Tuberculous meningitis occurs at any age and is currently more frequent in adults than children in the United States. Headache afflicts more than half the patients, a stiff neck is found in 75%, and lethargy, confusion, and fever are typical. The symptoms evolve more slowly in tuberculous than in bacterial meningitis, usually over a period of 1 to 2 weeks, but sometimes longer. This chronicity leads to frequent cranial nerve involvement, present in 20% of patients at the time of admission to the hospital. Spinal symptoms are uncommon, and both infarction and increased intracranial pressure are seen occasionally. Most patients with tuberculous meningitis have active tuberculosis elsewhere, although in some only inactive pulmonary lesions are found. The main distinction lies in the glucose level, which is reduced but not usually to the very low levels seen with bacterial meningitis. A more self-limited meningitis known as "serous meningitis" will develop in a few patients with a cerebral tuberculoma. The meningeal signs are mild and the symptoms tend to clear over a period of several weeks. However, it is possible for serous meningitis to progress to a more generalized (and fatal) tuberculous meningitis. The single most effective drug is isoniazid, but it has side effects (neuropathy and hepatitis) that can be disabling in alcoholics who may have these conditions from the outset. Neuropathy can be prevented by giving pyridoxine concomitantly, but hepatitis is not treatable except by discontinuing use of the drug. In patients taking ethambutol, optic neuropathy occasionally develops, so those receiving long-term ethambutol treatment should be screened at intervals for visual acuity and color discrimination. At times, an intracerebral tuberculoma requires resection if there is a mass effect or if it fails to shrink with drug therapy. Mortality is lower when treatment is started early, but it reaches 50% in patients in whom the condition is diagnosed while in coma. Despite the basal cistern loss caused by tuberculous meningitis, the associated hydrocephalus can be treated successfully in 70% of cases by endoscopic third ventriculostomy. Currently, the mortality rate for treated Haemophilus and meningococcal meningitis is 5% to 15% and has remained so for many years. Fulminant meningococcemia is possible with or without meningitis and has a very high mortality rate from vasomotor collapse associated with adrenocortical hemorrhage (Waterhouse-Friderichsen syndrome). The prognosis for bacterial meningitis is worse in those who have proven bacteremia, coma, seizures, and such concomitant disease as alcoholism and diabetes mellitus. Death occurs for a variety of reasons, including vascular collapse from septic shock, cerebral edema leading to transtonsillar herniation, respiratory failure secondary to aspiration pneumonia in an obtunded patient, and uncontrolled seizures. Those who recover from meningococcal meningitis usually show no residual deficits, but neurological injury occurs in 25% or more of children with Haemophilus meningitis and up to 30% of those with pneumococcal meningitis. In one study that monitored children after meningitis, 31% of those with pneumococcal meningitis had persistent sensorineural hearing loss, whereas the figures for meningococcal and Haemophilus meningitis were 10% and 6%, respectively. However, in developing countries, tuberculosis remains a very significant medical problem, and the lowering of barriers to immigration together with the increasing incidence of multidrug-resistant mycobacterial strains suggests that the case numbers are likely to rise in North America. Pathogenesis Tuberculous meningitis is caused by Mycobacterium tuberculosis in most patients and very occasionally by Mycobacterium bovis. Typically, it begins with bacterial seeding of the brain with the formation of tubercles that subsequently rupture and seed mycobacteria into the adjacent subarachnoid space. Such meningitis can be the terminal event in patients with miliary tuberculosis or occur less dangerously in the context of generalized tuberculosis with a single area of brain involvement. The accompanying exudate obliterates the basal cisterns and forms small white tubercles scattered throughout this area. Meningitis develops in about 25% of patients with syphilis, but it is generally asymptomatic and discoverable only by lumbar puncture. Rarely, it is manifested symptomatically as cranial nerve palsies, seizures, and increased intracranial pressure. Such meningitis may persist in the asymptomatic state or may subside spontaneously. Neurosyphilis always begins as a meningitis, but not all such meningitis progresses to vascular syphilis and the classic late phases of general paresis and tabes dorsalis. Syphilis is the most chronic form of meningitis affecting humans, and many of its associated pathologic changes may simply reflect the chronicity of the meningeal reaction. Factors leading to a transition from asymptomatic syphilitic meningitis to more symptomatic parenchymal neurosyphilitic forms are not known. However, treatment of asymptomatic syphilis is generally successful and will prevent such transformation. The course of the disease is quite variable from person to person, and presumably undefined immunologic factors temper the course of the disease. The abnormalities of spinal fluid seen in syphilitic meningitis include a pleocytosis of 200 to 300 cells/mm3, mainly lymphocytes and other mononuclear cells; elevation of total protein to 40 to 200 mg/dL; normal glucose content; and positive serologic tests. When they occur, symptoms are similar to those of other meningitides, and hydrocephalus may occur. However, unlike other forms of meningitis, patients with syphilitic meningitis are afebrile. Meningovascular syphilis is a more advanced form of the disease that usually occurs 6 to 8 years after the original infection. It should be considered when a relatively young person has one or more cerebral infarcts. Treatment still involves administration of penicillin as the drug of choice for all varieties of neurosyphilis, regardless of whether symptoms are present. The neurological involvement takes the form of a fluctuating meningoencephalitis or peripheral neuritis, or both. The meningitis is manifested as headache, stiff neck, nausea and vomiting, malaise, and chronic fatigue and fluctuates over a period of weeks to months. Cognitive and behavioral changes sometimes occur, as do seizures, ataxia, and choreiform movements, and cranial neuropathy is seen in half of patients, most frequently a facial palsy. Recommended treatment is high-dose penicillin (20 million units intravenously daily for 10 days) or ceftriaxone. Although many fungi can involve the nervous system, only a few do so with regularity and are listed in this section. The course of onset and the symptom profile of fungal meningitis are much like that of tuberculous meningitis, and the onset is insidious. As in other chronic meningitides, these patients are often afebrile and may have cranial nerve involvement, arteritis with thrombosis and infarction, and hydrocephalus. Cryptococcus is a fungus of the soil commonly carried by birds and transmitted to humans through the lungs or skin. The meningitis is granulomatous in nature, with granulomas containing fibroblasts, giant cells, areas of necrosis, and the organisms themselves. Its evolution is subacute, much like that of tuberculosis, but it may be fatal within a few weeks if left untreated. In some patients the course may be chronic, with the disease persisting for years in a waxing and waning course. No specific clinical features distinguish these forms from cryptococcal meningitis.
This is advantageous in that it may obviate the need for the surgeons and assistants to use standing stools antimicrobial bandages 250 mg arzomicin mastercard. In general, we try to position the operative field in as close to a horizontal plane as possible infection of the cervix discount 250 mg arzomicin mastercard. For lower cervical and cervicothoracic procedures, this often means that the patient must be placed in a considerable amount of reverse Trendelenburg positioning bacteria that causes pink eye buy arzomicin from india. The operating microscope can also improve surgeon comfort, as well as provide excellent illumination and magnification virus 360 generic arzomicin 250 mg. Particularly in the cervical region, its use can reduce surgeon discomfort during both anterior and posterior procedures virus respiratory generic arzomicin 100 mg with mastercard. An additional benefit is that the assistant has an excellent view of the procedure and can assist, if necessary. Inadequate cervical extension can make surgical access difficult and can result in a patient aligned in kyphosis postoperatively. Conversely, cervical hyperextension can exacerbate cervical spinal stenosis and place the patient at neurological risk intraoperatively. The Caspar head holder provides a flexible, adjustable means of placing patients in optimal alignment. A firm rubber chin strap maintains neutral head alignment, and a small adjustable pad is used to fine-tune the cervical lordosis. A small padded roll is placed underneath the patient and extended transversely to about the T2 level, and a foam doughnut is placed under the occiput. Paper tape extending from one side to the other and adherent to the forehead is adequate to maintain neutral alignment. Direct inspection is often the best method to detect whether this problem is in fact occurring intraoperatively. Again, we try to minimize the amount of force placed on implants and prefer to obtain optimal alignment through patient positioning. Finally, the importance of restoring or maintaining adequate lumbar lordosis has received much attention-and rightly so. Lumbar flexion facilitates decompressive lumbar laminectomy and lumbar microdiskectomy but should be assiduously avoided if an arthrodesis is to be performed. Use of the Wilson frame and a leg sling should generally be avoided in procedures that involve lumbar arthrodesis. Instead, we use modular hip and thigh pads on a spine table and a flat leg rest padded with pillows. SurgeonErgonomics An important and often overlooked aspect of patient positioning is to optimize the working environment for the surgeon. Particularly for long or difficult procedures, surgeon comfort should be considered carefully, although it should never assume priority PosteriorOccipitocervical,Cervical, Cervicothoracic As mentioned earlier, careful patient positioning for posterior cervical procedures is essential, particularly if an instrumented arthrodesis is to be performed. A modular spinal table with movable pads is, in our experience, preferable to other options for several reasons. First, unobstructed anteroposterior and lateral radiographs or fluoroscopy can be obtained. Second, the tabletop can be set up in a moderate reverse Trendelenburg position without raising the head unit. This allows the ideal position of the patient to be achieved without raising the patient excessively high, thereby avoiding the need for the surgeon to stand on steps during the procedure. We have found, however, that the patient must usually be moved to a stretcher before repositioning on the second table because the bulky table bases prevent them from being moved sufficiently close together to allow direct transfer of the patient from one table to the other. It is more efficient to use a modular spine table that allows the placement of a second tabletop and rotating the patient on the table. Adequate assistance must be available, but one individual should be in charge and delegate responsibility. We generally secure the head with Gardner-Wells tongs and 10 lb of in-line traction. For cervical procedures or if there is a concern about the cervical spine, we often also place a hard cervical collar on the patient. Perhaps it seems obvious, but it is important to remember that what is on top of the patient before rotation will be underneath the patient afterward. The surgeon should therefore ensure that adequate smooth padding is in place and that the patient will not be lying on intravenous lines or other noncompressible objects. Before rotating the patient, a final check should be made that the tabletops are secure, that all lines are disconnected and secured, and that everyone understands the direction of the rotation. The ventilator is disconnected, the patient is rotated, the table is secured, the ventilator is reconnected, and the upper tabletop is removed. It is also important to flex the knees and to ensure that the feet are in a relaxed, neutral position and not in forced plantar flexion. Positioning for procedures involving correction of complex coronal or sagittal deformities can be difficult. The most common situation is a patient with a significant thoracolumbar kyphosis or lumbar hypolordosis who is to undergo corrective osteotomies. For patients with fixed deformities, we position them in their natural (pathologic) alignment with a combination of built-up thoracolumbar supports and the leg sling. At the time of osteotomy closure and correction, the circulating nurse and an assistant will elevate the legs onto additional pillows, thereby increasing hip extension and helping to achieve correction. Anterolateral,RetropleuralThoracic, LateralLumbar Lateral positioning follows the same principles as for the more common anterior and posterior approaches. There is significant potential, however, for soft tissue or peripheral nerve injury secondary to focal pressure. Attention is therefore meticulously paid to these areas to ensure that adequate padding is used. A soft roll is placed under the dependent axilla to prevent excessive shoulder abduction and to distribute the pressure over a greater area. The dependent arm is externally rotated and the elbow is flexed to approximately 90 degrees. A folded pillow may be placed between the arms to keep them roughly parallel to the floor while allowing adequate access to the face. The dependent leg is flexed gently and the upper part of the leg is at most flexed slightly. Addition flexion may be helpful for lumbar flank approaches because it will tend to relax the iliopsoas and aid exposure. The common peroneal is susceptible to pressure injury as it crosses the proximal portion of the fibula just distal to the knee. The resultant orthogonal approach to the spine allows the surgeon to remain oriented to the location of the canal during decompression and placement of grafts and instrumentation. Asymmetric postoperative visual loss after spine surgery in the lateral decubitus position. The use of somatosensory evoked potentials to determine the relationship between patient positioning and impending upper extremity nerve injury during spine surgery: a retrospective analysis. Postoperative meralgia paresthetica after posterior spine surgery: incidence, risk factors, and clinical outcomes. AnteriorLumbar Positioning for anterior lumbar procedures is fairly straightforward. A small folded sheet or pad may be placed underneath the lumbar spine to enhance the lumbar lordosis and to bring the ventral aspect of the spine closer to the surgeon. It is important, however, to make certain that anatomic alignment is preserved if an anterior arthrodesis is performed. IntraoperativeRepositioning In some cases it is necessary or advantageous to perform "circumferential" surgery via different approaches on the same day. This requires intraoperative repositioning from a supine to a prone Full references can be found on Expert Consult @ Maniker In performing peripheral nerve surgery, as with any area of surgery, knowledge of the anatomy is of the utmost importance. The surgeon must not only understand the nerve anatomy but must also be able to correlate neural structures with their target muscles and sensory distribution. Knowledge of the vascular and bone anatomy will also be essential to planning the surgery. In much of nerve surgery, the normal anatomy is distorted-from trauma, tumor, or other disease-and the surgeon must have a clear anatomic picture of the normal anatomy before proceeding. A properly planned incision and exposure will allow the correct identification of the vital structures as well as room in which to perform the needed tasks. Although neurosurgeons are comfortable working in the small, confined spaces of the brain and spine, peripheral nerve surgery often allows the luxury of working in a more open, more exposed area. Whenever possible, exposure of a nerve should include normal proximal and distal nerve to allow the surgeon to work from the normal to the abnormal. The specific nerve or nerves to be operated on and the necessity of harvesting grafts will dictate much of the positioning for an operation. If intraoperative electromyographic monitoring of muscles is used, the limb may be draped out of the field. If, however, the observation of muscle contraction will be necessary and no monitoring will be used, either the entire limb must be exposed or clear plastic drapes should be available. In each case, the positioning and exposure must be worked out to suit the individual needs of the particular operation. More in-depth viewing of positioning for peripheral nerve surgery may be seen on Video 28-1. In the lower part of the posterior cervical triangle, after traversing between the anterior and middle scalene muscles, the C5 and C6 roots unite to form the upper trunk. Before this union, C5 gives off the dorsal scapular nerve to the rhomboids and a branch to the phrenic nerve. The C5 root, along with the C6 and C7 roots, gives off contributions to the long thoracic nerve to the serratus anterior muscle. The C7 root continues on as the middle trunk, and the C8 and T1 roots unite to form the lower trunk. The upper trunk gives off the suprascapular nerve to the supraspinatus and infraspinatus muscles as well as the nerve to the subclavius muscle. The divisions form at the level of the clavicle, and the cords continue into the infraclavicular space. The cords form just distal to the clavicle, below the tendinous insertion of the pectoralis minor muscle. The lateral cord gives off the lateral pectoral nerve and then terminates as the musculocutaneous nerve and the lateral contribution to the median nerve. The medial cord gives off the medial pectoral, medial brachial cutaneous, and medial antebrachial cutaneous nerves and then terminates as the ulnar nerve and the medial contribution to the median nerve. The posterior cord gives off the thoracodorsal and subscapular nerves and then terminates as the axillary and radial nerves. Although many variations have been reported, true anomalies of this basic anatomy are rare. Less often, C4 will contribute a branch to C5 (pre-fixed) and T2 will contribute a branch to T1 (post-fixed). The head is placed in a slight amount of extension and is turned 45 degrees to the contralateral side. Both lower extremities below the knee are sterilely prepared and draped to allow sural nerve harvesting for grafts. If other sources in the upper extremity, such as medial brachial and antebrachial cutaneous nerves, are to be used for grafting, the entire arm should be prepared. The surgeon should have the ability to work from superior to the clavicle and inferior to it. The arm board should be mobile enough to allow the surgeon to abduct or adduct the arm at the shoulder as necessary. Indications for this approach include a need for very proximal exposure to the neural foramina and the exiting nerve roots. This patient had previous radiation treatments to the anterior neck, making a traditional approach to the plexus not feasible. This approach will clearly expose the roots, trunks, and divisions but exposure for the cords and nerves is inadequate. As there is a greater potential for damage to the cupula pleurae of the lungs and a subsequent pneumothorax, the surgeon should have equipment for a chest tube on standby. An additional bolster should be placed under the patient at the level of the clavicle and upper sternum so that the anterior chest wall is lifted slightly off the operating table. For further details of this position and approach, the reader is directed to the paper published by Kline and associates3 or the text by Maniker. They can be combined for the full exposure of the plexus or tailored to expose the desired area of the plexus. The supraclavicular portion of the approach exposes the roots, trunks, and proximal portion of the divisions. The infraclavicular portion of the approach exposes the distal portion of the divisions, the cords, and the branches of the brachial plexus. The skin is then incised, and the interval between the biceps brachii and triceps is developed and the brachial fascia incised. This cadaveric exposure has had the clavicle removed for visualization, although it is not usually done in the living. Note that in this position, the surgeon may move from the posterior aspect of the patient to the anterior aspect of the patient to reach the radial nerve distal to the spiral groove. As there are no branches of the nerve in the arm, it is easily mobilized and traced both proximally and distally. An incision in a line connecting the acromion and olecranon, both of which are easily palpated, exposes the sulcus between the long and lateral heads of the triceps. Retraction of the superficial muscle exposes the radial nerve and profunda brachii artery. The radial nerve may then be traced distally as it passes from the posterior compartment into the anterior compartment of the arm.
The next section addresses the interactions of pathogens with this "inner defense antimicrobial door handles buy discount arzomicin 100 mg online. These cells were eventually termed microglia by Pio del Rio Hortega (1882-1945), who went on to further characterize these cells as a distinct entity in the brain parenchyma anabolic steroids best arzomicin 100 mg. Resting microglia are small cells with few surface markers and prominent thin branches that are constantly reorganizing and sampling the microenvironment of the brain parenchyma antibiotic used to treat bv discount arzomicin uk. Table 39-1 lists some of the cytokines and chemokines known to be generated by microglia in response to a number of activating stimuli oral antibiotics for acne minocycline arzomicin 250 mg lowest price. Multiple chemokine receptors have been identified in astrocytes, and ligation of these receptors has many downstream effects on astrocyte function, including regulation of chemokine production and receptor expression (Table 39-2) infection news discount 250 mg arzomicin fast delivery. Glutamate is an excitatory neurotransmitter that is highly neurotoxic, mainly via two mechanisms: (1) hyperactivation of neurons and (2) inhibition of cysteine uptake leading to oxidative damage to neurons through glutathione depletion. Streptococcus pneumoniae is a gram-positive bacterium responsible for a number of infections in humans, including pneumonia, otitis media, sinusitis, sepsis, and meningitis. A major component of this collateral damage involves brain edema, the development of ischemia, and neurotoxicity from elements of the immune response and from the invading pathogens themselves. Neurotoxicity includes direct cytotoxic insults to neurons from pathogen-derived factors. Scheld and colleagues monitored cerebrospinal hydrodynamics in rabbits during experimental meningitis by using a pressure device in direct continuity with the supracortical subarachnoid space. Experimental infection of rats with the encapsulated bacteria commonly responsible for human meningitis, S. Morphologic alterations of the blood-brain barrier with experimental meningitis in the rat. Pneumolysin lacks an aminoterminal signal sequence, which suggests that it is not secreted from pneumococci and requires autolysis for release. Hemolytic-uremic syndrome, the leading cause of acute renal failure in children, is highly associated with infection by Shiga toxin (Stx1 or Stx2)-producing E. Neurotoxicity can result from direct infection of neurons, from collateral damage secondary to the immune response, or from pathogen-derived factors that damage neurons during the infection. Some examples of broad neurotoxic mechanisms are discussed, followed by some examples of pathogen-specific mechanisms. Similarly, components of the cell wall and outer membrane of bacteria are capable of eliciting an intense inflammatory response bearing all the hallmarks of the meningitis produced by the whole bacteria themselves. A common finding of pneumococcal meningitis in animal models is the loss of neurons in the dentate gyrus of the hippocampus, predominantly via apoptosis. Intravenous administration of a glutamine synthetase inhibitor (l-methionine sulfoximine) to infected rabbits undergoing treatment with ceftriaxone significantly increased the density of apoptotic neurons in the dentate gyri of these animals when compared with rabbits receiving ceftriaxone alone. Grandgirard and coworkers examined differences in the inflammation associated with experimental pneumococcal meningitis treated with a lytic bactericidal antibiotic, ceftriaxone, and a nonlytic bactericidal antibiotic, daptomycin. These observations support the concept that release of bacterial products, through either autolysis or antibiotic lysis, contributes directly to the inflammatory damage associated with bacterial meningitis. BrainAbscess-PusintheParenchyma Brain abscesses are space-occupying purulent infections within the substance of the brain. The microbiology of brain abscess is predictably related to the primary source of the abscess; Table 39-3 lists microbes associated with specific primary sources. There is a predominance of streptococcal species and anaerobes associated with primary sources in the sinuses, mouth, and lung, whereas staphylococci and Enterobacteriaceae are commonly found in brain abscesses associated with direct inoculation from trauma or neurosurgical procedures. The time course of brain abscess development in humans has been characterized by computed tomography and in animal models via necropsy and histology. Brain abscess begins as an early cerebritis (days 1 to 3), with edema formation, tissue necrosis, and neutrophil infiltration. This early phase is followed by an intermediate to late cerebritis with infiltration of macrophages and lymphocytes, and this process culminates in the formation of a capsule infiltrated with plasma cells and myofibroblasts. Experimental study of the pathogenesis of brain abscess was significantly advanced with the development of a rat model of brain abscess. These important experiments demonstrate that microaerophilic and obligate anaerobes are probably not involved in the initiation of brain abscess despite the common isolation of these organisms from abscesses derived from different primary processes. The authors point out that this experimental model may not adequately reflect the initiation of brain abscesses in humans inasmuch as many of them are associated with mixed facultative aerobe/obligate anaerobe infections of the paranasal sinuses or dental structures, thereby leading to chronic exposure of the brain to mixed bacteria. Mixed facultative aerobe/obligate anaerobe infections are known to be synergistic in establishing infections at other sites in the body, and the clinical picture in human brain abscess probably reflects this synergistic advantage in establishing a brain abscess in normal human brain tissue. Before development of the rat brain abscess model, rhesus macaques (Macaca mulatta) were used to investigate the development and characteristics of brain abscesses in primates. Interestingly, abscesses in the animals injected intracerebrally developed thick capsules with an exuberant inflammatory response, beneficial prognostic features, whereas abscesses caused by "septic emboli" developed thin capsules, features historically associated with poorer clinical outcomes. Kielian and Hickey published the first study that examined the host cytokine response to rat brain abscesses induced by direct inoculation of S. These cytokine/chemokine/adhesion molecule changes agree well with the progression of brain abscess from an early, neutrophil-predominant cerebritis to an organizing lesion infiltrated with macrophages and lymphocytes. The importance of chemokines and neutrophils in the early inflammatory response to brain abscess was highlighted in a study using an S. Note the thin abscess wall with cavitation of infarcted tissue and the lackofamidlineshift. Cerebral abscesses produced by bacterial implantation and septic embolisation in primates. More evidence to support this "balance" hypothesis comes from observations on the effects of minocycline on experimental murine brain abscess. Thus, the clinical effects of drugs such as ciglitazone and minocycline on human brain abscesses deserve further investigation as adjuncts to surgical and chemotherapeutic interventions. As biotechnology progresses, more and more patients will have the privilege of experiencing "bionic" medicine in the form of implanted prosthetic devices. Perioperative contamination-either at the time of primary implantation or via manipulation at later times 2. Wound dehiscence over the shunt-with direct contamination at the erosion site and along the shunt tract 3. Hematogenous seeding-most clearly with intravascular devices, but it can occur with nonvascular devices 4. Distal port contamination-especially with ureteral drainage devices, but also with intraperitoneal and externalized devices Regardless of the mechanism of contamination, a common process that prevents subsequent sterilization of the shunt and often prompts removal of the device is the formation of bacterial biofilm. Notethedeposition of extracellular matrix, manifested as a complex web of material around and between microcolonies. Soon after placement, bioprosthetic materials are coated with host proteins, and these proteins may serve as receptors for adhesion molecules expressed by bacteria. Biofilms are complex surface structures consisting of sessile bacteria embedded in an extracellular matrix that is permeated by water channels. Quorum sensing itself is a complex set of processes that allow bacteria in a community to regulate the gene expression and phenotypes of other bacteria in the same community. Additionally, B, a global stress regulator, acts as a positive regulator of biofilm formation in S. Additionally, new chemotherapeutic interventions are needed; examples include bactericidal antimicrobials that penetrate biofilm and have a high threshold for the development of resistance, compounds that interfere with quorum sensing or transcriptional regulation of biofilm formation, or with both, and compounds that regulate phase variation among bacteria and drive sessile, biofilmed bacteria into the more susceptible planktonic form. Current concepts in the pathogenesis of meningitis caused by Streptococcus pneumoniae. Microglia as a pharmacological target in infectious and inflammatory diseases of the brain. Although mortality rates have decreased markedly, postcraniotomy infections commonly require prolonged antibiotic treatment and additional surgical interventions for successful eradication and frequently result in significant morbidity, prolonged hospitalization, and increased health care expenses. Many of the typical correlates of infection are nonspecific in the postoperative setting, and recognition of infection may frequently be delayed. An accurate understanding of the clinical, laboratory, and radiographic manifestations of postcraniotomy infection is critical to enable timely medical and surgical intervention and to limit the neurological sequelae of infection. This chapter examines these manifestations and discusses the tenets of effective therapy. The epidemiology of postcraniotomy infections is also discussed, along with a review of the factors conferring an increased risk for infection and the strategies that have proved to decrease the incidence of postoperative infection. Other bacteria frequently causing postcraniotomy infection included enterococci, Streptococcus spp. Yang and colleagues retrospectively identified 31 patients with brain abscesses after neurosurgical procedures and found gram-negative bacilli and polymicrobial infections to be the most frequent pathogens isolated. Earlier reports probably underestimated its pathologic role because of its often indolent clinical manifestation, as well as difficulties associated with microbiologic isolation of the organism, specifically the need for anaerobic culture held for 10 days. Although it is unlikely that all postoperative infections can be completely prevented, many of the factors influencing the development of infection may be modifiable, including those attributable to the patient and those related to the surgical intervention itself. Although the magnitude of contamination and the virulence of the contaminating organism certainly contribute to the rate of infection, all surgical wounds become inoculated with bacteria to some extent at the time of surgery, but in only a small percentage of patients does this contamination lead to clinical infection. Low levels of antibody and complement contribute to make the brain less efficient than other organs of the body at eradicating infection, and many of the underlying pathologies leading to neurosurgical intervention may significantly impair immune function. Deep organ space infections include subdural empyema, brain abscess, and meningitis/ventriculitis. Meningitis is the most common deep organ space infection and represents 22% of postcraniotomy infections, whereas other intracranial infections, including subdural empyema and brain abscess, account for 14% of infections. Several large prospective studies have reported infection rates ranging from 1% to 8%. Other frequent indications for craniotomy, such as trauma, have also been shown to be profoundly immunosuppressive. Several factors specific to craniotomy have been identified as increasing the risk for postoperative infection. Actual evidence demonstrating increased rates of infection with their use, however, is limited. Malliti and coauthors reported a nonsignificantly increased incidence of deep wound infections after craniotomy with the use of a nonresorbable polyester urethane synthetic dural graft (Neuro-Patch, B. The presence of nonresorbable dural substitutes may also impair the potential for an infected wound to be successfully treated because these grafts may become chronically colonized and could require removal to eradicate the infection. McCall and coworkers reported the uncomplicated use of several of these materials in a small number of patients in the setting of contaminated wounds, a finding suggesting that they may not impede clearance of infection. McGovern and coauthors reported a 29% rate of infection in cases associated with insertion of Gliadel wafers between 1996 and 1999. In general, the antibiotic chosen for prophylaxis should be safe, provide an appropriate narrow spectrum of coverage against relevant bacteria, and be administered for a defined, brief course. Additional perioperative factors that may potentially reduce the risk for postoperative infection include maintenance of normothermia and supplemental oxygenation. Several prospective randomized trials evaluating active warming of patients during colorectal surgery to maintain normothermia have shown decreased rates of infectious complications; the proposed mechanism of action is support of adequate blood flow and tissue oxygenation at the surgical site. Belda and colleagues conducted a prospective trial to evaluate the postoperative infection rate in patients randomized to receive either 30% oxygen or 80% oxygen during elective colorectal surgery. Studies evaluating the role of supplemental oxygen or temperature control for neurosurgical interventions have yet to be performed. Other perioperative risk reduction considerations include surgical site preparation and environmental control within the operating room. Failure to include an antibacterial agent with activity against the responsible bacterium may result in severe neurological sequelae or death. Antibiotic selection can be tailored once speciation and susceptibility testing from a microbiologic specimen are available. Administration of these agents in high doses achieves therapeutic concentrations within brain abscess cavities. Linezolid may be administered intravenously or orally and has excellent bioavailability. Experience with this agent for the treatment of postcraniotomy infections is limited, and potential side effects include reversible myelosuppression and irreversible peripheral neuropathy. Animal models of meningitis suggest that it may be an effective therapeutic agent in a setting of meningeal inflammation77-79; human studies to date are lacking. Rifampin is a broad-spectrum antimicrobial that may have a role in the adjunctive treatment of infections associated with foreign body implantation or bone flap osteomyelitis. These types of infections are notoriously difficult to eradicate because of their resistance to host defense mechanisms and poor penetration of antimicrobials. Most foreign body infections are caused by staphylococci growing in biofilms consisting of bacteria clustered together in an extracellular matrix attached to the foreign body. The number of health care workers within the operating room and traffic throughout the procedure should be kept to a minimum because bacterial shedding increases with activity and can potentially result in increased airborne contamination. Postoperative infections tend to be particularly difficult to resolve because of the complex anatomic changes resulting from craniotomy and the frequent involvement of virulent organisms. Early and decisive intervention is critical to limit morbidity, and the keystone of successful treatment is effective source control. The ability of antimicrobials to treat postcraniotomy infections successfully is a function of multiple factors. Selection of an antibiotic regimen should be based on the capacity of the antibiotic to penetrate the infected tissue effectively and to exhibit activity against the suspected pathogen. Bactericidal rather than bacteriostatic agents are generally preferred because of the inefficient opsonization and phagocytic capabilities within the brain. Inflammation at the site of infection may facilitate entry of drugs across these barriers and into the brain, but not all postoperative infections are accompanied by marked inflammation, and concomitant treatment with corticosteroids may further impair drug entry. Optimal antibiotic administration and dosing rely on an understanding of the pharmacodynamic properties of the agent and the susceptibility profile of the microorganism. In the absence of data from prospective randomized clinical trials evaluating the success rates of specific antibacterial agents, recommendations for the treatment of postcraniotomy infections are based largely on the results of previous experience, along with consideration of the complex physiologic, bacteriologic, and pharmacologic factors involved. Because of the rapid emergence of resistance, rifampin must always be used in combination with a second active agent. In vitro data, experimental animal models, and several randomized clinical trials suggest that dual therapy that includes rifampin may be better than monotherapy for orthopedic hardware related staphylococcal infections in terms of bone sterilization and cure rates.
250 mg arzomicin purchase free shipping. Novel Method for Rapid Antimicrobial Susceptibility Testing.
References
- Samuel KC. Atherosclerosis and occlusion of the internal carotid artery. J Pathol Bacteriol 1956;71:391.
- Mikawa K, Maekawa N, Goto R, et al: Use of prostaglandin E1 to treat peri-anaesthetic pulmonary hypertension associated with mitral valve disease, J Intern Med Res 21:161-164, 1993.
- Tsakiridis K, Mikroulis D, Didilis V, et al. Internal thoracic artery side branch ligation for post coronary surgery ischemia. Asian Cardiovasc Thorac Ann. 2007;15:339-41.
- Olivier A. Risk and benefit in the surgery of epilepsy: complications and positive results on seizures tendency and intellectual function. Act Neurol Scand (Suppl.) 117: 114-121, 1988.
- Pearce S, Colville RJI: Nailbed repair and patient satisfaction in children. Ann R Coll Surg Engl 92:483-485, 2010.
- Wolf, J.S., Monk, T.G. Anesthetic consideratios In: Smith, A.D., Badlani, G.H., Bagley, D.H. et al. Smith's Textbook of Endourology. St. Louis: Quality Medical Publishing; 1996, pp. 731-753.
- Kirby ML. Contribution of neural crest to heart and vessel morphology. In: Richard P Harvey, Nadia Rosenthal (Eds). Heart Development. San Diego, CA: Academic Press. 1999.