- info@careermakers.edu.np
- +977 1 4423870
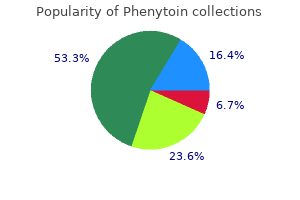
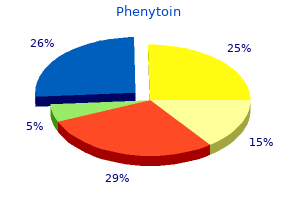
Phenytoin
Joanna Chikwe, MD
- Assistant Professor
- Department of Cardiothoracic Surgery
- Mount Sinai Medical Center
- New York, New York
These infants are more prone to develop aspiration of feeds and frequent lung infection treatment quadriceps strain phenytoin 100 mg without a prescription. Cry of the infant is weak and hoarse medicine reminder phenytoin 100 mg buy on line, breathing is labored and the air entry in lungs is reduced symptoms bronchitis order phenytoin 100 mg on line. In subglottic tracheal stenosis 340b medications discount phenytoin 100 mg buy on line, the cry is unaffected and the stridor is both inspiratory and expiratory medications emts can administer order 100 mg phenytoin overnight delivery. Angioma, papilloma, lymph angioma and retention cysts may be responsible for stridor. The left recurrent laryngeal nerve is more liable to injury since it has a longer course and hooks around the aorta from the front to back. Vascular rings cause intermittent stridor that becomes worse when the neck is flexed. Other causes of external airway compression are mediastinal goiter, lymphangioma and thyroglossal duct cyst. Congenital goiters which cause respiratory obstruction and stridor are due to maternal intake of antithyroid drugs and iodides during pregnancy. Goiter of neonatal hypothyroidism and that due to defect in the synthesis of thyroid hormones are usually not so big as to cause stridor. Other causes include micrognathia and glossoptosis, macro glossia and diaphragmatic hernia. Treatment the diagnosis of congenital laryngeal stridor can be established only by direct laryngoscopy. Fluoroscopy after barium swallow should be done to rule out the extrinsic causes of obstruction. Dyspnea Tachypnea refers to abnormally rapid respiration, while dyspnea means labored or difficult breathing, usually accompanied by pain and air hunger. The causes of dyspnea range from illnesses affecting the lungs, heart and musculoskeletal system. Epistaxis Epistaxis or bleeding from the nose is rare in children below the age of 3 yr. Systemic causes of epistaxis are: (i) hypertension, (ii) blood dyscrasia, (iii) emphysema, and (iv) pertussis. In resistant cases, the nasal mucosa is plugged with gauze piece soaked in 1:10,000 solution of adrenaline hydrochloride as a temporary measure. The bleeding points should be identi fied and cauterized with silver nitrate solution. The child should receive treatment with iron supplements to raise hemoglobin level. Profuse bleeding is more likely to be from the posterior aspect from sphenopalatine vessels. This is used for diagnosis of structural abnormality of airways, diagnosis of foreign body and for obtaining bronchoalveolar lavage samples to identify cell type and infective etiology of lower respiratory tract. This is commonly used for removal of foreign bodies from airways or obtaining biopsy from airway tumors. Estimation of partial pressures of oxygen (Pa02) and carbon dioxide (PaC02) in blood along with blood pH gives a fair estimate of pulmonary functions. Arterial blood gas analysis is useful in making a diagnosis of respiratory failure as well as for monitoring children with acute and chronic respiratory failure. Imaging Noninvasive diagnostic methods include X-rays, most commonly used to diagnose pulmonary infections and computerized tomography scans, used for visualization of lymph nodes, tumors, bronchiectasis and pleural pathologies. Sweat Chloride Test Chloride in sweat is increased in children suffering from cystic fibrosis. Nasal discharge may become purulent, if secondarily infected especially in younger children. Purulent discharge does not necessarily mean secondary infection as it can result from shedding of epithelial and inflammatory cells resulting from viral infection itself. Complications include otitis media, laryngitis, sinusitis, bronchiolitis, exacerbation of asthma and broncho pneumonia. Differential diagnosis include the presence of foreign body which presents with unilateral serosanguineous or purulent discharge from a nostril. Clear mucoid discharge from the nose in the first few weeks of life is called snuffles. Snuffles of congenital syphilis is severe rhinitis with bilateral serosanguineous discharge commonly excoriating the upper lip and leaving fine scars. Babies sneeze and blow out the nasal discharge, if their anterior nares are tickled by the tip of a handkerchief. These should not be used routinely and used only in refractory cases for limited duration. Antihistaminics are best avoided in the first six months of life, but give symptomatic relief by drying up thin secretions and relieving sneezing. Terfenadine should not be prescribed in children because of potential cardiotoxicity. If the cough is suppressed in infants and young children, mucoid secretions may be retained in the bronchi and this may predispose to spasmodic cough, wheezing, atelectasis and suppuration. These are used if the secretions become purulent, the fever continues to rise and if the child develops bronchopneumonia. The children should be protected from sudden exposure to chills and kept warm during the winter months. Acute Tonsillopharyngitis Sore throat is due to acute inflammation of the pharynx and tonsils. Most often, it is associated with the viral infections Common Cold or Nasopharyngitis Common cold is a frequent illness in childhood and is usually caused by infections of the upper respiratory tract with adenoviruses, influenza, rhinovirus, parainfluenza or respiratory syncytial viruses. Predisposing factors include chilling, sudden exposure to cold air and overcrowding. Clinical features of tonsillopharyngitis include fever, malaise, headache, nausea and sore throat. Younger children may not complain of sore throat but often refuse to feed normally. It is difficult to distinguish the clinical syndromes due to viral or streptococcal infections. In streptococcal infections, cervical lymph nodes are enlarged, the illness is acute with high fever and there is absence of nasal discharge or conjunctivitis. A possibility of acute pharyngitis due to group A beta hemolytic streptococci may be considered in a patient who has exudates in throat, tender enlarged cervical nodes along with absence of nasal or conjuctival congestion. Throat swab culture for group A beta-hemolytic strep to cocci helps in the definitive diagnosis. Complications of sore throat include acute glomerulo nephritis, rheumatic fever, otitis media, sinusitis and peritonsillar and retropharyngeal abscesses. The infection may spread down the tracheobronchial tree to cause tracheobronchitis and pneumonia. Differential Diagnosis Herpangina is an acute febrile illness due to group A Coxsackie virus. Patients have dysphagia, sore throat and papulovesicular lesions surrounded by erythema over the tongue, pharynx, anterior tonsillar pillars and soft palate. Diphtheria is characterized by moderate fever, severe toxemia, sore throat and membrane formation over the fauces or palate. Patients with pharyngoconjunctival fever have fever, conjunctivitis, pharyngitis and cervical lymphadenitis due to infection with adenovirus type 3. Infectious mononucleosis is characterized by lymphadenopathy, morbilliform rash, hepatosplenomegaly and sometimes, aseptic meningitis. Soft food such as custard or rice and lentil gruel is given because swallowing is painful. Where noncompliance is likely, a single intramuscular injection of benzathine penicillin (0. Cotrimoxazole, which is commonly used for sinusitis and otitis media, is not an appropriate medication for sore throat. Recurrent Sore Throat A detailed history is obtained and physical examination conducted. Dampness in the environment and overcrowding predispose the child to recurrent upper respiratory tract infections. Each episode of bacterial pharyngitis should be treated with adequate doses of antibiotics for at least 10 days. Presence of beta-lactamase producing bacteria in the pharynx may inactivate penicillin and lead to recurrent sore throat. In selected cases, penicillin prophylaxis may be administered for 3-6 months, especially if group A beta-hemolytic streptococcal infection is present. Tonsillectomy should be advised only if there are more than 5-6 episodes of tonsillitis in a year or tonsillar or peritonsillar abscess. It may reduce the incidence of infection with group A beta-hemolytic streptococcus. Tonsillectomy is recommended in diph theria carriers, in presence of retention cysts in tonsils or if the tonsils are a focus of infection for suppurative otitis media. There is no indication for tonsillectomy after rheumatic fever or glomerulonephritis. Metaanalysis of short course antibiotic treat ment for group A streptococcal tonsillopharyngitis. Inspiratory stridor, hoarseness or respiratory distress may not always be associated with croup. The diseases include acute epiglottitis, laryngitis, laryngotracheobronchitis and spasmodic laryngitis. Croup child becomes restless and anxious with fast breathing due to increasing hypoxemia. As the obstruction worsens, breath sounds may become inaudible and stridor may apparently decrease. This may unfortunately be misinterpreted as clinical improvement by an unwary physician. The child wakes up suddenly in the early hours of the morning with brassy cough and noisy breathing. Epiglottitis Supraglottitis includes both epiglottitis and inflammatory edema of the hypopharynx. Other microbes like pneu mococcus, beta-hemolytic Streptococcus and Staphylococcus are not common etiologies. The illness usually starts with a minor upper respiratory tract illness which progresses rapidly within the course of a few hours. The breathing becomes noisy but is generally softer than in case of laryngotracheobronchitis. The child is not able to phonate and often sits up leaning forwards with his neck extended and saliva dribbling from his chin which appears to be thrust forwards. The accessory muscles of respiration are active and there is marked suprasternal and subcostal retraction of the chest. The diagnosis of epiglottitis is made by a cautious direct laryngoscopy, wherein the epiglottis appears angry red and swollen. Injudicious attempt to examine the throat may, rarely, cause death by sudden reflex spasm of the larynx. It is therefore prudent not to force a child, panting for breath, to lie down for throat examination or to send him to the radiology department for an urgent X-ray film if the clinical diagnosis is other wise obvious. In case these procedures are considered essential, the equipment and personnel for respiratory resuscitation should always be readily available. Differential Diagnosis the syndromes of croup should be distinguished from each other and also from the croup associated with diphtheria in which a membrane is seen on laryngoscopy or occasionally with measles. As oxygen therapy masks cyanosis, a careful watch should be kept for impend ing respiratory failure. Fluids should be administered for adequate hydration of the patient by intravenous route. Endotracheal intubation or tracheostomy may be indicated if the response to antibiotics is not adequate and obstruction is worsening. A child with acute laryngotracheobronchitis should be assessed for severity of illness on basis of general appearance, stridor (audible with or without stethoscope), oxygen saturation and respiratory distress (Table 14. Mild cases can be managed on ambulatory basis with symptomatic treatment for fever and encouraging the child to take liquids orally. Parents may be explained about the progression of diseases and to bring the child back to hospital in case of worsening of symptoms. A patient with moderately severe illness may need hospitalization and treatment with nebulised epinephrine (1:1000 in doses of 0. While epinephrine acts rapidly to decrease vascular permeability, airway edema and improves Laryngitis and Laryngotracheobronchitis (Infectious croup) these conditions are nearly always caused by viral infections, usually with parainfluenza type l. Other viruses incriminated include respiratory syncytial and parainfluenza types 2 and 3, influenza virus, adenovirus and rhinovirus. Usually, there is a mild cold for a few days before the child develops a brassy cough and mild inspiratory stridor. As the obstruction increases, the stridor becomes more marked and the suprasternal and sternal recession with respiration become manifest. Severe croup may need hospitalization, preferably in intensive care, with oxygen inhalation and need for steroids (similar to moderate severity). Pneurnocystis jiroveci, his to plasmosis and coccidioidomycosis may cause pneumonia in immunocomprornised children. Other causes of pneumonia include ascaris, aspiration of food, oily nose drops, liquid paraffin and kerosene poisoning. Clinical Features Risk factors for pneumonia include low birth weight, malnutrition, vitamin A deficiency, lack of breastfeeding, passive smoking, large family size, family history of bronchitis, advanced birth order, crowding, young age and air pollution. Indoor air pollution is one of the major risk factor for acute lower respiratory tract infection in children in developing countries. Onset of pneumonia may be insidious starting with upper respiratory tract infection or may be acute with high fever, dyspnea and grunting respiration.
By dividing the soleus muscle along its attachment to the medial border of the tibia it is possible to expose the origin of the anterior tibial artery and the whole extent of the tibioperoneal trunk through this incision medicine clipart order phenytoin 100 mg with mastercard. If necessary medicine plus buy phenytoin 100 mg without a prescription, completely divide the medial head of gastrocnemius; this results in little functional disability medications 123 purchase 100 mg phenytoin overnight delivery. If you intend to perform a bypass with a saphenous vein graft treatment pneumonia buy phenytoin 100 mg without prescription, mark the vein before surgery; otherwise the incision should correspond with the anterior border of the sartorius muscle the tendency is to place this incision too anteriorly medicine ball workouts purchase 100 mg phenytoin with amex. Deepen the incision to expose the sartorius muscle, which is retracted posteriorly to reveal the neurovascular bundle enveloped by the popliteal fat pad. The artery lies on the bone and the nerve lies some distance away with the vein in between. The popliteal artery is always surrounded by a plexus of veins, which must be carefully separated and divided in order to avoid troublesome bleeding. To optimize exposure to this area the tendons of sartorius, semitendinosus and gracilis can be divided. If the greater saphenous vein is to be harvested identify the vein first along an appropriate length before Adductor magnus tendon 4 n If exposure of the whole length of the popliteal artery is required it is better to use a posterior approach. Deepen the incision through the popliteal fascia and fat pad and define the diamond between the hamstring muscles above and the two heads of gastrocnemius below; then follow the lesser saphenous vein in to the neurovascular bundle. In a posterior approach the popliteal artery will be superficial, with the vein and nerve lying deeper. Tibial arteries 1 n the proximal end of the anterior tibial artery is relatively inaccessible, but the remainder of this vessel and its terminal dorsalis pedis branch can be readily exposed through lateral or anterior incisions made directly over the vessels. Retract the tibialis anterior and extensor digitorum longus muscles anteriorly to reveal the artery lying on the interosseous membrane. If exposure of the proximal anterior tibial artery is required this can be achieved very effectively by excision of the upper part of the fibula with disarticulation of the proximal tibiofibular joint. The common peroneal nerve, which winds around the neck of the fibula, must be protected carefully. This approach destroys the lateral ligament of the knee and, while this is well tolerated in elderly, relatively immobile patients, it is best avoided in younger and fitter individuals. The peroneal artery lies directly deep to the fibula: it is accompanied only by vein and has Upper popliteal artery isolated between slings Sartorius muscle. In most cases, however, it is preferable to expose this vessel by a medial approach (see below). Cut edge of clavicular head of sternomastoid muscle Cut edge of scalenus anterior muscle Subclavian artery Brachial plexus 4 n To expose the peroneal artery by a medial approach, split the lat- on the medial aspect of the calf centred over the junction between gastrocnemius muscle and its Achilles tendon. Incise the deep fascia and develop the plane between the gastrocnemius and soleus muscles to reveal the posterior tibial vessels and nerve lying on the surface of soleus beneath a layer of fascia. Alternatively, the posterior tibial artery and its terminal lateral plantar branch may be exposed by an incision made directly over it, as it lies behind the medial malleolus where it is covered only by deep fascia, and then following it in to the foot. This reveals the artery surrounded by its concomitant veins in the depths of the wound. Subclavian artery 1 n Make a transverse incision 1 cm above the medial third of the clavicle; divide the platysma muscle in the same plane. This exposes the clavicular head of the sternocleidomastoid muscle, which is divided, and also a fat pad containing the scalene lymph nodes. Dissect and retract this fat pad superiorly off the surface of the scalenus anterior muscle. Identify the phrenic nerve, which passes obliquely from lateral to medial across the front of this muscle to lie along the medial border of its tendon and usually separated from it by a few millimetres. Retraction of the muscle superiorly exposes the subclavian artery with its vertebral, internal mammary and thyrocervical branches. The first thoracic nerve root and the lower trunk of the brachial plexus cross the first rib above and posterolateral to the artery. The subclavian vein is deep to the clavicle and is not normally seen through this approach. On the left side the thoracic duct enters the confluence of the internal jugular and subclavian veins. If it is damaged, ligate it to prevent the development of a troublesome postoperative chylous fistula. On the rare occasions when direct exposure is considered essential this is best achieved by splitting the manubrium and upper sternum. Make a right-angled incision with a horizontal component above the medial third of the clavicle and a vertical component in the midline over the manubrium and upper sternum. The periosteum is extremely vascular and diathermy is required to seal the small arteries. Commencing at the suprasternal notch, open a retrosternal plane by finger dissection, and then, with a sternal chisel and hammer or a properly protected reciprocating saw, divide the manubrium and sternum in the midline and spread the edges with a self-retaining retractor. Dissection of the thymus and anterior mediastinal fat is necessary to expose the arch of the aorta and the origins of the supra-aortic vessels. The innominate vein is stretched across the upper part of the incision and must be protected. It is not usually necessary to excision of the inner two-thirds of the clavicle, although this is rarely necessary. The two most common operations on the subclavian artery are carotid-subclavian anastomosis or bypass for a proximal occlusion (subclavian steal syndrome) and repair of a subclavian aneurysm (this is usually a misnomer since most so-called subclavian aneurysms involve the first part of the axillary artery). The former is usually completed without difficulty through the approach described above, and the latter is most conveniently accomplished with separate incisions above and below the clavicle to expose the subclavian and axillary arteries (see below). Posterior tibial artery and concominant veins Soleus muscle Gastrocnemicus muscle Achilles tendon. Close with peristernal wire or strong nylon sutures, taking care to avoid damage to the internal mammary and intercostal arteries when inserting them. The origin of the left subclavian artery, which arises far back on the aortic arch, can also be exposed through a posterolateral thoracotomy through the bed of the second or third ribs. For an axillofemoral bypass procedure consider placing the arm in abduction to facilitate estimating the length of the graft required. Make a horizontal incision 1 cm below the lateral third of the clavicle, and split the fibres of pectoralis major muscle. This exposes the infraclavicular fat pad, beneath which lies the pectoralis minor muscle. Divide the tendon of this muscle close to its origin at the tip of the acromion process. Find the axillary artery surrounded by the cords of the brachial plexus, which must be carefully protected. The axillary artery can be a friable vessel and care should be taken when slings and clamps are applied. Care should also be taken when performing an anastomosis that the back wall of the artery is not inadvertently incorporated in to the suture line. At this point it is still enclosed by cords of the brachial plexus joining to form the median nerve, which crosses it obliquely from the lateral to the medial side. Median nerve Brachial artery Biceps tendon Ulnar artery Radial artery 2 n the proximal brachial artery is found in the groove between bi- 3 n It is more frequently necessary to expose the bifurcation of the Axillary artery with lateral and medial cords of the brachial plexus Pectoralis minor muscle (divided) embolectomy. Distal extension of this incision permits the radial, ulnar and anterior interosseous arteries to be followed in to the forearm. However, it is useful at this point to summarize the range of procedures available: trauma 1 n Direct repair, interposition grafting and patch grafting for arterial n 3 n Thrombolytic therapy, percutaneous suction and mechanical 2 Surgical embolectomy or thrombectomy embolectomy n Split fibres of pectoralis major muscle 368. The basic technique involves the use of a guide-wire and a balloon dilatation catheter. None of these has yet found a major role in the routine management of vascular disease, and lasers in particular, despite increasing technological sophistication, have so far proved disappointing. The use of balloon catheters (some with drug elution) has, however, made a major impact in recent years and in vascular centres the majority of patients with occlusive disease are treated by these methods reconstruction, for example in the pedal arteries, is a valuable sign and there are a number of simple and inexpensive devices available to supplement clinical assessment, including strain gauge and photoplethysmographs (digital pulse monitors), toe temperature probes, flat and hand-held Dopplers and pulse oximeters. Technique of percutaneous transluminal angioplasty with the Gruntzig balloon catheter. Omission of this step results in a high incidence of early postoperative occlusion and is therefore unacceptable. It is important to appreciate that the presence of a palpable pulse in a graft gives no indication whatsoever that it is technically satisfactory. There may be no mean forward flow through the graft and yet it will be pulsatile to palpation. Acceptable methods available for assessing vascular reconstructions at operation include the following: method. Place an X-ray plate wrapped within a sterile Mayo tray cover directly beneath the limb, and take an exposure while injecting 1520 ml of contrast medium in to the proximal end of the graft. Apply a clamp proximal to the injection site during exposure to obviate the necessity for accurate timing of the exposure. Observe proper radiation protection measures during this procedure and further reduce the radiation dose to yourself by interposing a long length of connecting catheter (for example an arterial line) between the syringe and the injection site. For more proximal reconstructions, special X-ray equipment is required but other methods of quality control may be effective. It is also possible to use a simple hand-held Doppler probe placed in a finger of a sterile surgical glove with gel to assess flow. Although the relevance of each varies according to specific circumstances it is a valuable discipline to include an appraisal of all three factors when planning any arterial reconstruction: n An unimpeded inflow tract the run-in. Under these circumstances there is a danger that the symptoms of ischaemia may be masked and therefore go unrecognized until irreversible tissue damage has occurred. Always assess the distal circulation in cases of fractured long bones or disarticulation injuries, especially those that involve the elbow or knee. Occlusion of a single tibial or forearm vessel is usually tolerated without ischaemic damage and does not as a rule require reconstruction. Inserted at one end, such instruments will allow direct inspection of the interior of a graft and anastomosis. However, such instruments traumatize the flow surface and are expensive and for these reasons have been largely abandoned. It is true that the smooth muscle of arteries contracts protectively in response to injury so that an important vessel may appear quite small both angiographically and on direct inspection. Assess 1 n On entering the haematoma there may be brisk fresh bleeding, in 2 n If there is complete disruption of the artery find the ends and ap3 n the traumatized vessel will be damaged some distance proxiply soft clamps. In the case of limb injuries this is either the original arsels distal to the site of injury. The procedure must include measures to deal with this problem (see below), otherwise the run-off vessels are usually normal. Since only short segments are required, problems are rarely encountered in finding a vein of suitable quality and calibre. If there has been extensive injury to both artery and major veins consider harvesting a segment of vein from the opposite leg or upper limb. Repair of damaged major arteries always takes precedence over orthopaedic fixation of fractures. However, there is a danger that vascular anastomoses may disrupted during subsequent manipulation of fractures. In these circumstances it may be advisable to restore vascular continuity initially by inserting a temporary intraluminal plastic shunt, and completing the repair once the fractures have been stabilized, when the length of the arterial defect can be accurately measured. Attempt direct end-to-end anasto- 5 n If the artery is in continuity there may be bruising of the adven- mosis only if there will be no tension. In most cases it is more prudent to insert an interposition graft of autologous vein, even if this is only a centimetre in length. The intima and inner layers of the media split transversely and the edges roll back to form a flap, which obstructs flow, causing secondary thrombosis. It is never sufficient, therefore, to simply inspect the outer surface of such a vessel and it is totally unacceptable to treat such lesions by topical application of vasodilator substances. Excise the damaged segment completely, cutting back each end of the artery as before to find healthy intima. If either is inadequate pass a Fogarty catheter distally and proximally to withdraw any propagated clot and then instil heparinized saline. Prepare 1 n Once the presence of major arterial injury has been established, n undertake surgical exploration without delay. Inform the blood bank of major haemorrhage so that appropriate products can be made available. This requires a skin incision that extends well beyond the confines of the injury. Remember to reverse the vein to avoid obstruction to blood flow by competent valves. Complete the proximal anastomosis first, in end-to-end fashion, using the triangulation technique with interrupted sutures for small or inaccessible vessels or the oblique overlap technique for larger vessels. Apply a clamp to the distal end of the graft and allow arterial pressure to distend it in order to determine the optimum length to avoid both excessive tension and kinking. Technical difficulty may be encountered in effecting satisfactory end-to-end anastomoses, usually because of awkward access. Under these circumstances the ends of the artery may be ligated and the area of trauma bypassed with end-to-side anastomoses at remote, more accessible, sites. If there is any doubt about the effectiveness of the repair, obtain an on-table angiogram. Recurrent thrombosis despite a technically satisfactory repair warrants immediate systemic heparinization. It may be difficult to decide whether or not to repair associated damage to veins. As a rule, repair major axial veins such as the femoral vein and, in the case of nearamputation of a limb, restore continuity to two veins for each artery repaired. Where primary closure is either not possible or inadvisable, always cover the arterial repair with healthy viable tissue, which in practice usually means a muscle flap.
Simple fluoroscopy without contrast is usually sufficient to guide this manoeuvre symptoms high blood sugar buy online phenytoin, but if persistent difficulty is encountered obtain a road-map by injection of contrast through the needle symptoms job disease skin infections order phenytoin 100 mg visa. Never pass a hydrophilic guide-wire through a metallic needle: the hydrophilic coating will be stripped off by the needle when the wire is withdrawn symptoms 9dpo bfp cheap phenytoin 100 mg, with potentially dire consequences symptoms liver cancer 100 mg phenytoin. Be aware that this technique may be used concurrently with open arterial reconstruction (for example harrison internal medicine order phenytoin 100 mg otc, iliac angioplasty and femorodistal bypass). An introducer sheath is always used and permits repeated endovascular access with minimal trauma to the vessel. The size of sheath required is determined by the procedure to follow balloon angioplasty usually requires a 47F sheath; stent placement may require a larger catheter. All manufacturers recommend the appropriate sheaths on their instructions and packaging. Place a pursestring suture of 5/0 polypropylene (Prolene) around the artery before puncturing the vessel directly with a Potts-Cournand needle. Flush the sheath with heparinized saline through the side channel, which is fitted with a tap. This channel can also be used for injection of contrast medium in order to obtain an angiographic image of the lesion. The size of guide-wire required is indicated on the packaging of the balloon catheter most often 0. Introduce it through the sheath floppy end first, using the small plastic introducer cone that comes with the wire to penetrate the valve. Always wipe the guide-wire with a swab soaked in heparinized saline after removing a catheter as dried blood on the surface obstructs the smooth passage of a subsequent catheter. Inject a small amount of local anaesthetic at the chosen puncture site and make a nick in the skin with a no. While palpating the common femoral artery with the fingers of one hand introduce a Potts-Cournand or similar needle. Angle the needle to facilitate access of the guide wire in the direction required and to avoid puncture of the back wall or creation of a false lumen and dissection. For infrainguinal procedures, puncture the artery just distal to the inguinal ligament, allowing room to manoeuvre the tip of the needle within the lumen of the common femoral artery whilst negotiating the guide wire in to the superficial femoral artery. Note that the inguinal ligament lies approximately 2 cm proximal to the groin crease. Care should be taken to identify the landmarks accurately in all patients: do not be misled in obese patients whose groin crease will be significantly lower than the inguinal ligament. For access to the upstream iliac arteries the puncture site may be a little lower, but take care to avoid unintended puncture of the superficial or profunda femoris arteries. When no pulse is palpable or percutaneous access is difficult use an ultrasound-guided arterial puncture technique. Unless there is severe inflow obstruction, the absence of pulsatile flow from the needle indicates that the tip is not properly positioned within the lumen. Do not attempt to advance a guide wire, but re-position the needle to gain access to the arterial lumen. For accurate sizing of the balloon obtain an angiogram using a measuring catheter with 1 cm markings. However, this degree of precision is not normally necessary: for lesions in the superficial femoral artery balloons with a diameter of 6 mm, and for iliac lesions 8 mm, are usually appropriate. A guide-wire that is within the lumen passes without resistance: if resistance is encountered do not apply force as this is likely to result in dissection of the subintimal plane. For pressure of 510 atmospheres with a 50/50 mixture of contrast medium and saline. It is not necessary to maintain inflation of the balloon for more than a few seconds but a second inflation helps smooth the irregularities of the flow surface that result from splitting and fissuring of the plaque. Re- 19 n Following withdrawal of the introducer sheath apply digital pres- member that some irregularity of the flow surface at the site of angioplasty is usual. If a significant stenosis remains, or if a large intimal flap has developed following iliac artery angioplasty, consider the use of an intraluminal stent. Stents do not perform well in arteries below the groin and should only be used in exceptional circumstances. Give clear instructions to the nursing staff regarding duration of bed rest prior to mobilization to minimize haematoma and pseudoaneurysm formation. If the artery has been exposed, tie the purse-string suture to secure haemostasis or apply clamps and proceed with the open procedure. Monitor peripheral perfusion and the groin for signs of haematoma or formation of a false aneurysm. The femoral vein lies medially and must be protected, but the femoral nerve on the lateral side lies in a deeper plane and is not usually at risk. However, do not be over zealous with positioning of a self-retainer, as the nerve can easily be stretched and a neuropraxia ensues. Gently lift the artery with the sling and identify its branches and its bifurcation in to the superficial and profunda femoral arteries. Take care to avoid damage to the profunda vein, a tributary of which always passes anterior to the main stem of the profunda artery. For a more extensive exposure of the profunda femoris artery divide this vein between ties. There is no sure way of avoiding this, but approach the artery from its lateral rather than its medial side and gently reflect any lymph nodes and visible lymph vessels off the femoral sheath with minimal damage. If there are any obvious lymph leaks at the time of surgery suture the lymphatic channels closed with 6/0 Prolene. La technique operatoire des anastomoses vasculaires et de la transplantation des visceres. Prior to embarking on this surgery decide which part of the artery needs to be accessed and consider how the patient should be positioned on the operating table. The vein is exposed first and this has to be lifted carefully away to give access to the artery. Prepare 1 n the urgency of the situation dictates that preoperative preparation must be limited. Aftercare n 2 n Arrange regular half-hourly observation of the distal circulation 1 Except in cases where continued bleeding is a serious problem, maintain anticoagulation with heparin for several days. Access 1 n For lower limb emboli, expose the common femoral artery (see 2 n For upper limb emboli, expose the brachial artery in the antecubital fossa (see above). Complications 1 n Early thrombosis or bleeding at the site of the repair demands im2 n A false aneurysm may result from a contained anastomotic leak 3 n the risk of associated deep venous thrombosis is high, so take apand this also requires early re-exploration and repair. In the case of the femoral 2 n Select an embolectomy catheter of a size appropriate to the vessel: 3 n A number of different makes of embolectomy catheter are avail3F for axillary and brachial arteries, 4F for the superficial and profunda femoral arteries and 5F for the aortic bifurcation. Choose one with a central irrigating lumen that permits injection of heparinized saline or X-ray contrast medium in to the vessels beyond the balloon. Inflate the balloon and withdraw the catheter slowly while adjusting the pressure within the balloon to accommodate changes in the diameter of the vessel. Avoid severe friction between the balloon and the arterial wall since this can cause intimal damage to the vessel. Directly suture the common femoral artery; consider using a small vein patch for the brachial artery. Prepare 1 n Prior to the administration of thrombolytic therapy it is mandatory to ascertain that patients have no contraindication to it. Haemorrhagic pathologies, bleeding tendency, recent surgery and intracardiac thrombus are a few of the contraindications. The catheter will not pass proximally or forceful forward bleeding is not obtained. This can be due to pre-existing arterial disease or to the catheter having been introduced in a subintimal plane. Avoid direct aorto-iliac reconstruction under these circumstances if at all possible and perform either a femoro-femoral crossover or an axillofemoral bypass. This may show embolus impacted at the popliteal bifurcation and in the tibial arteries, or evidence of atherosclerotic occlusion. Alternatively, expose the infrageniculate popliteal artery to enable Fogarty catheters to be introduced directly in to the tibial vessels. If there is a longstanding atherosclerotic occlusion of the superficial femoral artery, restoration of blood flow to the profunda system alone is likely to be sufficient to save the limb. However, if distal perfusion remains poor, then proceed to femoropopliteal bypass. Where facilities for intra-operative fluoroscopy exist, as an alternative to exposure of the popliteal artery for retrieval of emboli from the tibial arteries, pass the embolectomy catheter over a guide-wire negotiated in to each vessel in turn. Action 1 n Puncture the common femoral artery with a Potts-Cournand nee- n 3 n Under X-ray control advance a long guide-wire through the vessel beyond the embolus. Because the agent is infused locally in to the thrombus relatively small amounts are required. The high incidence of serious bleeding complications associated with systemic administration is thereby reduced. This involves pulsed high-pressure injection of the thrombolytic agent through a catheter with multiple side holes. Lysis may occur over a period of hours or may need to continue for 2448 hours, with repeated angiography to assess progress and repositioning of the wires. This requires close nursing supervision of the patient, with fastidious care of the intraarterial lines and infusions. This avoids haemorrhagic complications and is associated with a reduced risk of embolization of fragmented thrombus in to the peripheral vascular bed. The most effective device employs the Bernouilli effect to break up and aspirate the thrombus. In most cases adjuvant percutaneous angioplasty will be necessary to deal with causative stenotic lesions due to anastomotic intimal hyperplasia or progressive atheroma. Ensure a graft takes its blood supply from an area of the aorta with adequate inflow and assess and consider the position of the proximal clamp, especially in the presence of calcified plaque which may be at risk of rupture. Further administration of the thrombolytic agent may be effective but it must be infused directly in to the clot. Alternatively, small fragments may be removed by suction applied to a larger catheter (suction embolectomy). Provided that the viability of the limb has been secured, small residual fragments of this type may be of no consequence and they may lyse spontaneously. The profunda femoris artery is nearly always patent but may be stenosed at its origin. There is evidence that the long-term patency of aortofemoral grafts is affected adversely when only one of the run-off vessels is patent. In all other patients it is probably better to confine the operation to the proximal bypass initially and then appraise the merits of a second distal bypass at a later date. However, always correct any profunda origin stenosis at the time of aortofemoral bypass. Use a bifurcated polyester Dacron graft either 14 mm  7mm, 16 mm  8 mm or 18 mm  9 mm, depending on the diameter of the native vessels. Complications 1 n In order to minimize haemorrhagic complications, monitor coagulation tests repeatedly and adjust the dose of thrombolytic agent accordingly. Prepare 1 n the major risk associated with aortic surgery is that of cardiac complications. It is, therefore, appropriate for patients to undergo cardiac risk assessment before surgery. This might include evaluation of myocardial perfusion, measurement of leftventricular ejection fraction and coronary angiography. It is imperative that any arterial lines in situ have continuous infusions to prevent clot formation. Fibrinolytic treatment of residual thrombus after catheter embolectomy for severe lower limb ischaemia. These will be described in detail here and will not be repeated in subsequent sections. Appraise 1 n the indications for aortobifemoral bypass have decreased con- Cover the genitalia with a small towel and apply an adhesive drape allowing access to the whole of the abdomen and both inguinal regions. When only one intra-abdominal arterial anastomosis is anticipated, as, for example, in an aortobifemoral bypass, a transverse incision made directly over 4 n Manage extensive unilateral iliac disease by either a unilateral extraperitoneal bypass or a femoro-femoral crossover graft (see below). The segment between the renal vein and the inferior mesenteric artery is usually the most favourable. Stomach, transverse colon and omentum packed superiorly Left renal vein Duodenum Small bowel packed to the right Descending colon Aorta 2 n If there is a total occlusion of the aorta, it is most appropriate 3 n Assess the inferior mesenteric artery. If it is a large vessel with a widely patent aortic ostium then preserve it carefully. If the aorta is not totally occluded then many surgeons prefer to construct an end-to-side (onlay) anastomosis in order to preserve perfusion through the natural vessels in to the internal iliac arteries. If the external iliac arteries are occluded then an endto-side anastomosis is preferred as there may be no retrograde flow from the distal anastomoses in to the iliac system, and ischaemia of the pelvic organs and buttocks may otherwise ensue. Action 1 n In order to perform the proximal anastomosis choose an aortic clamp to either occlude the aorta completely, by applying a straight aortic clamp vertically down the sides of the aorta to the spine or by partially occluding the aorta and creating a window anteriorly through which an arteriotomy is performed. In occlusive disease there may be numerous collaterals, so take care not to damage these. If the occlusive disease is close to the take off of the renal arteries then consider gaining suprarenal control by exposing and gaining control of the aorta below the diaphragm. This is achieved by dissecting adjacent to the lesser curve of the stomach, taking care to avoid damage to the oesophagus. Make the incision 2 cm above the umbilicus and extend 23 cm beyond the rectus sheath on each side. Open the posterior rectus sheath and the peritoneum together; vessels in the edge of the falciform ligament should be ligated. A self-retaining retractor system such as Omnitract allows the bowel to be retained within the abdomen, protected by large moistened abdominal packs behind retractor blades. Dissection in the subintimal plane carries a risk of obstruction of the renal arteries by an intimal flap and must be avoided at all costs.
Roseola should be differen tiated from childhood illnesses such as rubella ad medicine order phenytoin without a prescription, measles 86 treatment ideas practical strategies buy phenytoin online, enteroviruses and drug hypersensitivity treatment 3rd degree heart block 100 mg phenytoin buy otc. Infectious mononucleosis should be differentiated from other causes of mononucleosis like illness treatment yeast infection child order discount phenytoin online, streptococcal pharyngitis and acute leukemia symptoms tonsillitis cheap phenytoin 100 mg on-line. This virus has tropism for cells of the erythroid lineage at the pronormoblast stage. Transmission of infection is by the respiratory route and the incubation period is 4-28 days (average 16-17 days). The prodromal phase is mild and consists of low-grade fever, headache and symptoms of mild upper respiratory tract infection. It spreads rapidly to the trunk and proximal extremities as a diffuse erythematous macular rash that rapidly undergoes central clearing to give it a lacy or reticulated pattern. Complications include arthropathy, idiopathic thrombocytopenic purpura and aseptic meningitis. Fifth disease should be differentiated from measles, roseola, rubella and drug rash. Other serious manifestations of parvovirus B19 infection include arthralgia and arthropathy in adolescents or adults, transient aplastic crises in patients with chronic hemolytic anemias, chronic anemia, pancytopenia or marrow suppression, virus associated hemophagocytic Treatment Rest and symptomatic therapy are advised. Participation in strenuous activities and contact sports should be prohibited in the first 2-3 weeks of illness due to risk of splenic rupture. This presents as earache, jaw tenderness while chewing, dryness of mouth and swelling at the angle of jaw. Occasionally, other salivary glands, including the submaxillary and sublingual glands, are affected. The occurrence of epididymoorchitis is more common in adolescent boys or postpubertal men. Other neurological manifestations include auditory nerve damage leading to deafness, cerebellar ataxia, facial neuritis, transverse myelitis and Guillain-Barre syndrome. Mumps parotitis needs to be differentiated from suppurative parotitis, submandibular lymphadenitis, recurrent juvenile parotitis, calculus in Stensen duct and other viral infections causing parotitis. Mumps Mumps is an acute viral infection characterized by painful enlargement of the salivary glands, most characteristically the parotid glands. The virus is spread from human reservoir by direct contact, air-borne droplets and fomites contaminated by saliva and urine. The virus proliferates in the respiratory epithelium to enter the circulation and then gets localized to the glandular and neural tissue. The virus has been isolated from saliva as long as 6 days before to 9 days after appearance of salivary gland swelling. Treatment Symptomatic treatment is given in the form of antipyretics and warm saline mouthwashes. Steroids may be used for symp to matic relief of orchitis and arthritis but does not alter the course of disease. Prevention the affected patient should be isolated until the parotid swelling has subsided. Mumps Poliomyelitis the polioviruses belong to the genus Enterovirus in the family Picornaviridae and comprise three related - Essential Pediatrics serotypes: types 1, 2 and 3, all of which can cause paralysis. Type 1 is most frequently responsible, type 3 is less commonly causative and type 2 is only rarely implicated. Epidemiology the disease is seasonal, occurring more commonly in summer and early autumn in temperate climates. Feco-oral route is the predominant mode of transmission in developing countries with poor sanitation, whereas oral-pharyngeal transmission predominates in industrialized countries and during outbreaks. Humans are the only reservoir of poliovirus and infec tion is spread from person-to-person. Transmission is usually widespread in the community by the time of onset of paralysis in a child. Infants born to mothers with antibodies are protected naturally against paralytic disease for a few weeks. Immunity is acquired through infection with the wild virus and through immunization. The initiative was hugely successful with reduction of polio cases from 350,000 worldwide in 1988 to 650 in 2011 and only 215 cases in 2012 (as of 25th December 2012). The last wild polio case was reported from India on 13 January, 2011 and India is no more considered endemic for poliovirus. The virus is usually present in the pharynx and stools before the onset of paralytic illness. It invades local lymphoid tissue, enters the bloodstream to invade certain nerve cells and may damage or destroy these cells. Symptoms occur in two phases, minor and major, separated by several days without symptoms. The major phase of illness begins with muscle pain, spasms and the return of fever. This is followed by rapid onset of flaccid paralysis that is usually complete within 72 hr. Severe cases may deve lop quadriplegia and paralysis of the trunk, abdominal and thoracic muscles. Paralysis in extremities begins proximally and progresses to involve distal muscle groups. Depending on the strain of poliovirus, the ratio between subclinical and clinical cases is estimated to range between 100:1 and 1000:l. Residual Paralysis Following an acute phase of illness lasting 1-4 weeks, the recovery of paralyzed muscles begins. The extent of recovery is variable ranging from mild to severe residual paresis at 60 days, depending upon the extent of damage caused to the neurons by the virus. After two year, no more recovery is expected and the child is said to have postpolio residual paralysis, which persists throughout life. Current serologic tests cannot differentiate between wild and vaccine virus strains. Eradication of Polio Eradication is possible because polio affects only man, immunity is lifelong, a safe vaccine is available and there are no carriers or reservoirs of the infection. The strategies for achieving this goal are: Attaining high rntes of routine immunization. When poliovirus transmission is reduced to well-defined and focal geographic areas, intensive house-to-house, child-to-child immunization campaigns are conducted over a period of days to break the final chains of virus transmission. Other conditions with a presentation similar to those of paralytic poliomyelitis include traumatic neuritis and less fre quently, meningitis, encephalitis and illnesses produced by toxins (diphtheria, botulism) (see Chapter 19). Treatment Treatment should be early and appropriate to the stage and degree of paralysis. Children with bulbospinal polio and respiratory paralysis require hospitalization. In the acute stage, children with isolated paralysis of one or more limbs can be managed at home. They should be advised complete rest, proper positioning of the affected limb and passive range of movement at the joints. Massage and intra muscular injection should be avoided during acute phase of illness. The child should be made to lie on a firm bed and maintain limbs in neutral position. Warm moist fomentations can be given with soft towels, dipped in warm water to relieve pain and spasms. This helps to stimulate proprioceptive impulses from muscles and tendons, helping improve muscle power. As the acute phase of illness subsides, recovery in muscle power is helped by giving physiotherapy, helping ambulation and prevention of deformities. Prevention of Poliomyelitis the available vaccines and the recommended schedule are discussed in Chapter 9. Hand-Foot-Mouth Disease Hand-foot-mouth disease is a common viral illness primarily affecting children below 5 yr. The most common causes of hand foot mouth disease are coxsackie virus A16 and enterovirus 71. The disease usually presents as outbreaks, often in preschool children and transmission is by direct contact with an affected patient or infected fomites. Hepatitis A and E are responsible for most of the water-borne (community acquired) hepatitis while B, C and D are responsible for post-transfusion hepatitis. Hence, it spreads readily by the feco-oral route through contaminated food and water and from person-to-person living with poor sanitation. Symptomatic disease is uncommon and outbreaks rare in developing countries with poor hygiene since most individuals are infected in childhood. In regions with intermediate endemicity like India, a significant proportion of people escapes infection in childhood and may develop symptomatic disease as adults. Clinical Features the onset is with a prodrome characterized by low grade fever, feeling of being unwell and sore throat. This is followed by development of ulcers or blisters in the oral cavity, mostly on the posterior aspect and then a papulovesicular skin rash on the palms and soles and less commonly, on buttocks, knees, elbows and genital area. Complications include temporary loss of toe nails or finger nails about 4 weeks after onset of disease. Rare complications include aseptic meningitis, encephalitis, polio like paralysis, myocarditis and respiratory distress syndrome. Outbreaks, particularly due to enterovirus 71, are reported from China, Vietnam, Taiwan and Malaysia, in which neurologic complications are common and mortality significant. Some experts believe that entero viruses cause hand-foot-mouth disease now occupy the ecologic niche vacated by eradication of polioviruses. Diagnosis is clinical and requires differentiation from other illnesses causing oral ulcers like herpangina, herpetic gingivostomatitis and aphthous ulcers and from chicken pox. Treatment and Prevention Treatment is mainly symptomatic and includes analgesics and soft diet. Isolation of affected children at home and promotion of hand hygiene to prevent disease spread is important. This is followed by a short prodromal phase lasting up to a week, which is characterized by loss of appetite, fatigue, abdominal pain, nausea and vomiting, fever, diarrhea, dark urine and pale stools. In this case, high fever, marked abdominal pain, vomiting, jaundice and the development of hepatic encephalopathy associated with coma and seizures occur. In patients who survive, neither functional nor pathologic sequelae are common despite the widespread necrosis. Its titer increases over 4-6 weeks, then declines to nondetectable levels within 6 months of infection. Laboratory evaluation of liver function includes estimation of total and direct bilirubin, transaminases, alkaline phosphatase, prothrombin time, total protein and albumin. There is no evidence to suggest that restriction of fats has any beneficial effect on the course of the disease. Antiviral agents have no role because the hepatic injury appears to be immunologically mediated. Referral to a liver transplant center is appropriate for patients with fulminant hepatitis. Acute hepatitis is marked by symptoms similar to other acute hepatitis illnesses, i. Fulminant hepatitis is heralded by pathologic mental status changes within 2 to 8 weeks after the initial symptoms in an otherwise healthy child. Although liver damage is usually mild during childhood, serious sequelae, including cirrhosis and hepatocellular carcinoma, may develop insidiously at any age. If adminis tered within two weeks of exposure it either prevents development of disease or reduces its severity. Epidemiological transition of hepatitis A in India: issues for vaccination in developing countries. In areas of low endemicity, horizontal infection is the main route of transmission. During the early phase of infection, the amount of virus in the liver and blood is usually large, whereas the liver damage is mostly mild. The host immune system gradually recognizes the virus and starts to clear the virus. It results in active inflammation of the liver and elevation of serum aminotransferases. Interferons are a group of naturally occurring agents with antiviral, antineoplastic and immunomodulatory properties. Lamivudine monotherapy for 1 yr provides satisfactory results in children with chronic hepatitis B. The medication is well tolerated, has minimal side effects and is easy to administer. The viral genotypic distribution in children generally parallels that reported regionally in adults. Enzyme immunoassay is limited by frequent false-positive results, particularly in patients with elevated globulin levels such as those with autoimmune hepatitis. Longer-acting pegylated inter ferons have been subsequently developed based on the premise that more sustained drug levels would result in greater antiviral activity. Importantly, biochemical and virologic responses have been accompanied by significant histologic improvement in all treated patients included in these trials, and interferon has been well tolerated in children. Treatment of children persistently infected with hepatitis B virus: seroconversion or suppression.
Prevention and Control the patient should be isolated until two successive cultures of throat and nose are negative for diphtheria bacillus symptoms narcolepsy phenytoin 100 mg without prescription. All household and other contacts should be observed carefully for development of active lesions medications requiring aims testing generic phenytoin 100 mg overnight delivery, cultured for C medicine zoloft discount phenytoin 100 mg buy online. Previously immunized asymptomatic patients should receive a booster dose of diphtheria toxoid symptoms 6dp5dt purchase 100 mg phenytoin. Those not fully immunized should receive immunization for their age (see Chapter 9) medicine x boston buy discount phenytoin 100 mg line. It may affect any susceptible host but is more common and serious in infancy and early childhood. The worldwide prevalence of the illness has declined following widespread vaccination. Protection against typical disease wanes 3-5 yr after vaccination and is unmeasurable after 12 yr. Specific diagnosis depends on isolation of the organism from nasopharyngeal swab or cough plate cultured on Bordet-Gengou medium, which is often positive in the catarrhal and paroxysmal stage. Other conditions that present with prolonged episodes of spasmodic cough include adenoviral infection, endo bronchial tuberculosis, inhaled foreign body and reactive airway disease. The initial manifestations are indistin guishable from upper respiratory tract infections. Unlike the upper respiratory infections, the cough does not improve in a few days but becomes more severe and frequent with the passage of time. Though the cough may not be typically paroxysmal in early stages, it tends to be annoying and frequent at night. The paroxysmal nature of the cough is suspected towards the latter part of this phase. The paroxysmal stage lasts for 2-6 weeks in which cough progresses to episodic paroxysms of increasing intensity ending with high-pitched inspiratory whoop. The whoop is produced by the air rushing in during inspiration through the half-open glottis. The whoop may not always be present in infants who present with apneic or cyanotic spells. Repeated thrusting of tongue over the teeth causes ulceration of the frenulum of the tongue. In the convalescent phase the intensity and paroxysms of cough decrease gradually over 1-4 weeks. Management General measures include providing adequate nutrition and hydration and avoiding factors aggravating cough. Nebulization with salbutamol is effective in reducing bronchospasm and controlling bouts of cough. As enteric fever is a disease transmitted by the feco-oral route, its greatest burden is in resource limited countries where water supply and sanitary conditions are poor. Enteric fever is the most common cause of fever lasting for more than 7 days in clinical practice in India. The organism must Diagnosis the diagnosis of whooping cough is based on clinical features. On reaching the small intestine, the organism penetrates the mucosa and infects the lymphoid follicles and subsequently the draining mesenteric lymph nodes and the liver and spleen. It multiplies in the reticuloendothelial system and after incubation period varying from 7 to 14 days spills in to the bloodstream and is widely disseminated, especially to liver, spleen, bone marrow, gallbladder and the Peyers patches of the terminal ileum. Infection leads to both local and systemic immune responses, which are, however, inadequate to prevent relapse or reinfection. It is higher with beta lactams such as cefixime or ceftriaxone as compared to quinolones and azithromycin. These individuals are potential sources of infection for family members and contacts and for the community if they are in occupations that involve food-processing. There is no data on carrier prevalence in children and routine culture of stool following recovery from enteric fever is not recommended. Diagnosis There is no appreciable difference between the manifestations of typhoid and paratyphoid fever. This pattern differentiates it from viral fever where the peak is usually at the onset of fever. With fever, there is associated malaise, dull headache, anorexia, nausea, poorly localized abdominal discomfort, mild cough and malaise. Physical findings are unremarkable with the exception of a coated tongue, tumid abdomen and sometimes hepatosplenomegaly. The rash described in Western textbooks is seldom or never seen in Indian subjects. Infants and young children with enteric fever may have diarrhea as a predominant manifestation or a short-lasting undifferentiated febrile illness. In the absence of treatment fever may continue for 3-4 weeks followed by natural remission or by development of complications. Bleeding is due to erosion of a necrotic Peyers patch through the wall of a vessel and is usually mild but can, sometimes, be life-threatening. Perforation is a dreaded complication manifesting as acute abdomen, with high mortality unless appropriately treated. Other complications of enteric fever include splenic abscesses, hepatitis, cholecystitis, pneumonia, disseminated intra vascular coagulation and other manifestations such as psychosis, ataxia or meningitis. Leukocyte counts may be normal to low with absolute eosinopenia and neutrophilic predominance. Sufficient blood should be collected (10 ml in adults and 5 ml in children) and a blood: media ratio of 1:5 should be maintained. Bone marrow cultures have higher yield as compared to peripheral blood cultures as Salmonella is a pathogen of the reticuloendothelial system and should be done when patients present in later stages of the illness. The Widal test detects presence of IgG and IgM anti bodies to H(flagellar antigen) of S. Anti O titers are both IgG and IgM that rise and decline early, while anti H are primarily IgG that rise and decline late in course of the disease. The conventional method of interpretation of the Widal test has been to demonstrate four-fold rise in antibody titers in two samples. The sensitivity of the test is low in the first week of illness and in patients treated with prior antibiotics. Specificity is low owing to anamnestic reactions, prior vaccination, cross reactivity with other Enterobacteriaceae and subclinical infections in endemic areas. Other tests such as Tubex and Typhidot that detect IgM antibodies against typhoid have not proven superior to the Widal test. Infections and Infestations - enteric fever can be managed at home with oral antibiotics and advice to seek medical followup in case of failure to respond to therapy or development of complications. Children with persistent vomiting, inability to take orally, severe diarrhea or abdominal distension usually require intravenous antibiotics therapy and intravenous fluids, necessitating admission to hospital. Fluoroquinolones, introduced in the late 1980s and early 1990s, produced very good results initially, but the past decade has seen a progressive increase in the minimum inhibitory concen trations of ciprofloxacin in S. Now that the susceptibility breakpoints have been revised downwards, this discor dance between in vitro and in vivo susceptibility will be resort. Resistance to nalidixic acid has been suggested as a marker of fluoroquinolone failure. Currently, third-generation cephalosporins such as ceftriaxone and cefixime are the first-line agents for therapy of enteric fever. In patients with history of penicillin or cephalosporin allergy, aztreonam, chloramphenicol (in higher than usual doses) or cotrimoxazole (in higher than usual doses) are used as second-line agents. Parenteral treatment is continued until defervescence has occurred, oral intake has improved and complications resolved. Thereafter, therapy can be switched to oral cefixime to complete a total duration of 14 days. Other oral drugs that may be used for switch over therapy include cefpodoxime, azithromycin, cotrimoxazole and amoxicillin. However, the experience with cefpodoxime is limited and the other agents require switch to a different class of antimicrobials than cephalosporins. If cultures are positive and show quinolone resistance as well as sensitivity to other drugs ampicillin, chloramphenicol and cotrimoxazole), it is prudent to continue with ceftriaxone alone rather than change because the older drugs do not offer any advantage over ceftriaxone. If cultures are negative and defervescence has not occurred by day 7, a thorough search for alternative etiology for fever should be made and ceftriaxone continued. There is no role for changing the antimicrobial agent or adding another drug, since ceftriaxone resistance is still anecdotal. The choice of medication depends on individual preference, experience and level of comfort and cost considerations. There is no data at present to support use of combination therapy in enteric fever. Therapy of relapses Relapse rates vary with the type of drug and are most common with beta lactams (ceftriaxone, cefixime) especially if shorter duration of therapy is used. Usually relapses may be satisfactorily treated with the same drug as used for primary therapy but at appropriate dose and duration. However, if the isolate is quinolone sensitive and fluoroquinolones were not used for primary therapy, they should be used for treatment of the relapse. Therapy of carriers the carrier state is uncommon in children and testing for chronic carriage 3 months after an episode of enteric fever is not recommended. If the strain is nalidixic acid sensitive, quinolones for 28 days is a better option. Prevention the most effective and desirable method for preventing enteric fever is by improving hygiene and sanitation. This will yield additional dividends of reduction in the burden of other water-borne illnesses as well. While rats are the principal source of human infection, dogs, cats, livestock and wild animals are other reservoirs. The survival of excreted organisms depends on the moisture content and temperature of the soil. Humans acquire infection after getting exposure to water or soil contaminated with rat urine. Agricultural workers, veterinarians, meat handlers, rodent control workers and laboratory personnel are at risk of getting infected because of occupational exposure. During the immune phase, some children develop aseptic meningitis or uveitis with recurrence of fever. In icteric Ieptospirosis (Weil syndrome) after the initial phase of fever patients develop severe hepatic and renal dysfunction. All patients have abnormal urinary finding on urinalysis in the form of hematuria, proteinuria and casts. Hemorrhagic manifestations are rare but when present, may include epistaxis, hemoptysis and gastrointestinal and adrenal hemorrhage. Diagnosis Complete blood count shows anemia, leukocytosis with polymorph predominance and thrombocytopenia. In patients with Weil disease there is elevated serum creatinine, deranged coagulation parameters and direct hyper bilirubinemia with raised transaminases. Specific diagnosis is established by serologic testing, microscopic demonstration of the organism or culture. Cross reactivity and false positivity is seen with other infections like enteric fever and malaria. Demonstration of organism in tissues or urine by dark field microscopy or immunoflorescence and cultures are not routinely available. Leptospirosis should be differentiated from other febrile illnesses commonly seen in the monsoon season like malaria, dengue, enteric fever, acute viral hepatitis and hantavirus infections. Pathogenesis Leptospira enter the body through abrasions and cuts in skin or through mucous membranes and spread to all organs hematogenously. The organisms damage the endothelial lining of small blood vessels, with leakage and extravasation of blood cells, hemorrhage and ischemic damage to various organs including liver, kidneys, meninges and muscles. Clinical Features Human infection ranges from asymptomatic infection to a severe multiorgan involvement which is often fatal. In the initial or septicemic phase lasting 2-7 days, the onset is abrupt with high grade fever with rigors and chills, lethargy, severe myalgia, headache, nausea, vomiting. Some patients develop acute respiratory distress syndrome with respiratory failure. In some patients, after a brief asymptomatic phase, the second phase, called the immune or leptospiruric phase, becomes manifest where Leptospira localize to tissues to cause specific signs and symptoms. For oral treatment amoxicillin and doxycycline (in children above 8 yr) are the drugs of choice. Single dose doxycyline or amoxicillin following Infections and Infestations - exposure can prevent illness but is not routinely recommended. Recovery from tetanus occurs by sprouting new nerve terminals in the spinal cord leading to relaxation of the contracted muscles. Tetanus Tetanus is caused by the bacterium Clostridium tetani, a spore forming, anerobic, gram-positive motile bacillus, found in human and animal feces. Tetanus commonly occurs in areas where soil is cultivated, in rural areas, in warm climates and during summer months. The spores of the organism remain nonpathogenic in soil or contaminated tissues until conditions are favorable for transformation in to vegetative form. Transformation occurs in the presence of locally decreased oxygen reduction potential, typically in devitalized tissue, in the presence of a foreign body, trauma and crush injury and suppurative infections. Tetanospasmin, is the main toxin responsible for the manifestations of the disease. Pregnant women who are not immunized against tetanus do not pass on protective antibodies to their babies. Infection results of unhygienic birth practices, most commonly when the umbilical cord is contaminated at the time of cutting after delivery. Symptoms usually appear by the third day afterbirth, never in the first two days of life and rarely after the age of two weeks.
Order phenytoin 100 mg otc. Eye Flu : Cause Symptoms & Prevention By R. S. Dawas (Naturopath).
References
- McNeal JE: Normal histology of the prostate, Am J Surg Pathol 12(8):619n633, 1988.
- Donovan JL, Kay HE, Peters TH, et al: Using the ICSQoL to measure the impact of lower urinary tract symptoms on quality of life: evidence from the ICS-iBPHi Study. International Continence SocietyoBenign Prostatic Hyperplasia, Br J Urol 80(5):712n721, 1997.
- Beguin S, Mardiguian J, Lindhout T, et al: The mode of action of low molecular weight heparin preparation (PK10169) and two of its major components on thrombin generation in plasma, Thromb Haemost 61:30, 1989.
- Miner JR, Heegaard W, Plummer D: End-tidal carbon dioxide monitoring during procedural sedation. Acad Emerg Med 9:275, 2002.
- Payne WS, Fisher J: Esophageal reconstruction: Free jejunal transfer or circulatory augmentation of pedicled interpositions using microvascular surgery. In Delarue NC, Wilkins EW Jr, Wong J, editors: International trends in general thoracic surgery, Vol. IV, Esophageal cancer. St. Louis, C.V., 1988, Mosby. 31.