- info@careermakers.edu.np
- +977 1 4423870
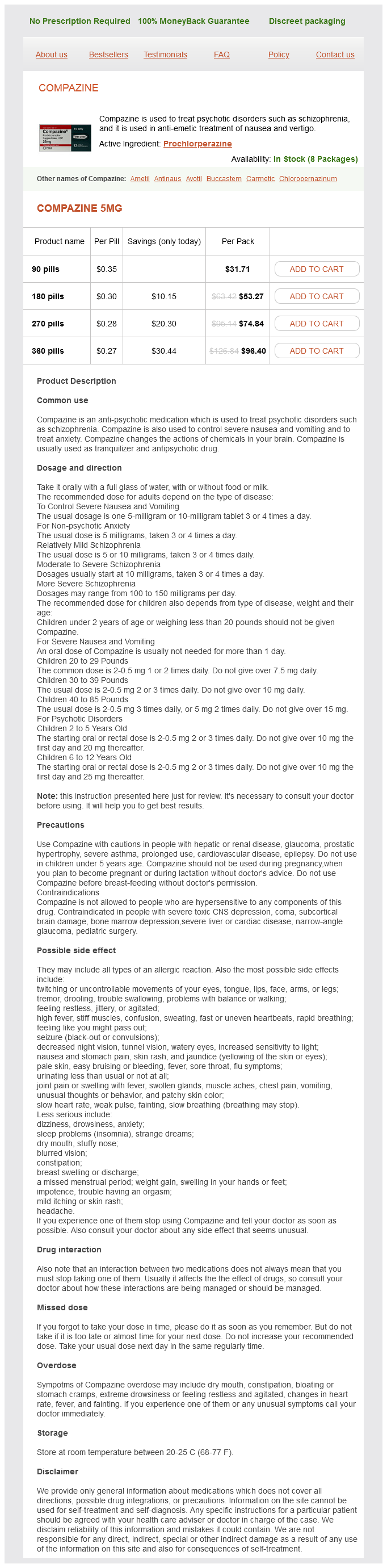
Prochlorperazine
Joanne M. Bargman, MD, FRCPC
- Professor of Medicine, Faculty of Medicine, University of
- Toronto
- Staff Nephrologist, Department of Medicine,
- University Health Network, Toronto, Ontario, Canada
- Non-infectious Complications of Peritoneal Dialysis
Changes in regional cerebral blood flow during acute electroconvulsive therapy in patients with depression medicine look up drugs order prochlorperazine with a mastercard. Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis treatment definition cheap prochlorperazine on line. Occurence of ultra-rapid cycling during electroconvulsive therapy in bipolar depression medications journal purchase prochlorperazine 5 mg with amex. An examination of mortality and other adverse events related to electroconvulsive therapy using a national adverse event report system treatment wasp stings order prochlorperazine 5 mg without prescription. Chapter Novel non-invasive brain stimulation approaches for treatment-resistant mood disorders Andrй Russowsky Brunoni medications similar to gabapentin prochlorperazine 5 mg buy overnight delivery, Pedro Shiozawa, and Felipe Fregni. Introduction the use of electricity as a treatment for psychiatric disorders is not new. However, the controlled use of electric currents for medical disorders only began in the eighteenth century, with the development of the voltaic pile, even though the use of electric currents for the management of mental disorders was still limited and empirical. Response to fluoxetine was associated with a marked reduction in local cerebral blood flow as well as changes in downstream limbic and cortical sites as measured with positron emission tomography (Mayberg et al. The effects of chronic deep brain stimulation for patients with refractory depression have also been investigated. Primary outcome revealed a significant clinical effect considering remission rates (4. On the other hand, Fregni and colleagues (2006c) showed that age and treatment refractoriness were significant independent negative predictors of depression improvement. Other potential adverse effects are rare and include syncope episodes due to vasodepressor-related mechanisms, headaches, and acute psychiatric changes, such as treatment-emergent affective switches. Repetitive transcranial magnetic stimulation should not be performed in cases whenever metal devices are present anywhere in the head. Pregnancy has to be analysed individually for each case since precise safety considerations have not been established. A recent open-label study involved participants with treatment-resistant bipolar depression. Overall, no significant differences were observed regarding clinical efficacy in these subgroups. Depression improvement is the score change in from baseline to endpoint, for each study. The treatment was well withstood by all participants and significant adverse effects were not observed. High-frequency repetitive transcranial magnetic stimulation accelerates and enhances the clinical response to antidepressants in major depression: a meta-analysis of randomized, double-blind, and sham-controlled trials. A randomized, double-blind clinical trial on the efficacy of cortical direct current stimulation for the treatment of major depression. A randomized double-blind sham-controlled study of transcranial direct current stimulation for treatment-resistant major depression. Gray matter abnormalities in Major Depressive Disorder: A meta-analysis of voxel based morphometry studies. The Sertraline versus Electrical Current Therapy for Treating Depression Clinical Study: Results from a factorial, randomized, controlled trial. Long-term efficacy after acute augmentative repetitive transcranial magnetic stimulation in bipolar depression: a -year follow-up study. Transcranial magnetic stimulation in patients with bipolar depression: a double blind, controlled study. Pilot study of the clinical and cognitive effects of high-frequency magnetic seizure therapy in major depressive disorder. Cognitive effects of repeated sessions of transcranial direct current stimulation in patients with depression. Predictors of antidepressant response in clinical trials of transcranial magnetic stimulation. Daily left prefrontal transcranial magnetic stimulation therapy for major depressive disorder: a sham-controlled randomized trial. Transcranial direct current stimulation in the treatment of major depression: a meta-analysis. Repetitive transcranial magnetic stimulation for treatment-resistant depression: a systematic review and metaanalysis. Daily left prefrontal repetitive transcranial magnetic stimulation in the acute treatment of major depression: clinical predictors of outcome in a multisite, randomized controlled clinical trial. Transcranial direct current stimulation for depression: 3-week, randomised, sham-controlled trial. A double-blind, sham-controlled trial of transcranial direct current stimulation for the treatment of depression. Regional metabolic effects of fluoxetine in major depression: serial changes and relationship to clinical response. Transcranial direct current stimulation in treatment resistant depression: a randomized double-blind, placebo-controlled study. Rapid-rate transcranial magnetic stimulation of left dorsolateral prefrontal cortex in drug-resistant depression. Maintenance transcranial magnetic stimulation reduces depression relapse: A propensity-adjusted analysis. Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Nosce the ipsum: On the efficacy of transcranial magnetic stimulation in major depressive disorder. Antidepressant effects of sertraline associated with volume increases in dorsolateral prefrontal cortex. Treatment-emergent mania in unipolar and bipolar depression: focus on repetitive transcranial magnetic stimulation. Image showing location of implanted pulse generator in the chest and of the electrode around the left vagus nerve. The electrical stimulation parameters, which include current, pulse width, frequency, and duty cycle (percentage of time stimulation is delivered), are controlled via a telemetry device which communicates with the implanted pulse generator. Dorr and Debonnel reported that stimulation of the vagus nerve in rats resulted in increased firing rates of neurons in the locus coeruleus and the dorsal raphe nucleus, structures involved in noradrenergic and serotonergic neurotransmission, respectively (2006). However, more recent studies have failed to replicate this association (Bajbouj et al. The medium and high groups demonstrated more sustained antidepressant responses and less frequent suicide attempts than the low-dose group. The reported rates of adverse psychiatric events have included hospitalization due to worsening of the depression (2. Adjustable parameters, such as pulse width, frequency, and amplitude, can be modified by the treating physician, and titrated to clinical effect. Preclinical and neurophysiologic studies have demonstrated that these conditions are driven by dysfunction in key motor-circuit structures governing voluntary human behaviour (Hutchison et al. The risk of hemorrhage or stroke is approximately Â2 per cent with half of these resulting in neurologic impairment (Hamani et al. In addition, there is an up to 9 per cent risk of post-operative complications, including infection, hardware malfunction, or stimulation-associated adverse events (Hamani et al. The latter can be managed with modification of stimulation parameters, and are commonly reversible. The Papez circuit postulated that limbic structures exist in an interconnected network linking cortical structures, such as the hippocampus and cingulate, with deeper subcortical structures, such as the thalamus. Dysfunction in the circuit or any of its components may lead to disturbances in mood. Since then, knowledge about the circuit has been significantly modified and expanded. Top-down influences on mood, such as expectations, reward contingencies, and executive functioning, all of which are affected in depression, are governed by typically medial frontal structures such as the prefrontal cortex and anterior cingulate (Mayberg, 997; Pizzagalli, 20). Bottom-up influences, such as more vegetative functions including sleep, sex drive, and metabolic rate, also affected in depression, are governed by subcortical structures, including the amygdala, hypothalamus, and brainstem (Pizzagalli, 20). Both influences appear to converge on key modulatory structures such as the peri- and sub-callosal cingulate and insula, which serve to modulate and regulate inputs and feed back to centres that influence behaviour. For example, work done by Mayberg and colleagues has shown that both induced sadness in healthy control subjects, and baseline sadness in depressed patients, are associated with hyperactivity of the subcallosal cingulate (Mayberg, 997). Puidgemont and colleagues reported a 63 per cent response rate at one -year, and a 50 per cent remission rate at the same follow-up (Puigdemount et al. Vagus nerve stimulation therapy randomized to different amounts of electrical charge for treatment-resistant depression: acute and chronic effects. A patient-level meta-analysis of studies evaluating vagus nerve stimulation therapy for treatment-resistant depression. These promising results support the idea that targeting a key structure in the hedonic pathway may offer relief to patients suffering from this particular symptom of their illness. Nucleus accumbens deep brain stimulation decreases ratings of depression and anxiety in treatment-resistant depression. Long-term effects of nucleus accumbens deep brain stimulation in treatment-resistant depression: evidence for sustained efficacy. Effect of vagus nerve stimulation on cerebrospinal fluid monoamine metabolites, norepinephrine, and gamma-aminobutyric acid concentrations in depressed patients. Life Expectancy at Birth for People with Serious Mental Illness and Other Major Disorders from a Secondary Mental Health Care Case Register in London. Vagus nerve stimulation for chronic major depressive disorder: 2-month outcomes in highly treatment-refractory patients. Association of cerebral metabolic activity changes with vagus nerve stimulation antidepressant response in treatment-resistant depression. Brain blood-flow change with acute vagus nerve stimulation in treatment-refractory major depressive disorder. Vagus nerve stimulation is associated with mood improvements in epilepsy patients. Treatment resistant depression as a failure of brain homeostatic mechanisms: implications for deep brain stimulation. Acute blood flow changes and efficacy of vagus nerve stimulation in partial epilepsy. Subcallosal cingulate deep brain stimulation for treatment-resistant unipolar and bipolar depression. A multicenter pilot study of subcallosal cingulate area deep brain stimulation for treatment-resistant depression. Subcallosal cingulate gyrus deep brain stimulation for treatment-resistant depression. Systematic review and meta-analysis of vagus nerve stimulation in the treatment of depression: variable results based on study designs. Reduced limbic connections may contraindicate subgenual cingulate deep brain stimulation for intractable depression. Vagus nerve stimulation: 2-year outcomes for bipolar versus unipolar treatment-resistant depression. Mortality and suicide risk in treatment-resistant depression: an observational study of the long-term impact of intervention. Frontocingulate dysfunction in depression: toward biomarkers of treatment response. Deep brain stimulation of the subcallosal cingulate gyrus: further evidence in treatment-resistant major depression. Neurostimulation therapies for treatment resistant depression: a focus on vagus nerve stimulation and deep brain stimulation. Effects of 2 months of vagus nerve stimulation in treatment-resistant depression: a naturalistic study. Deep brain stimulation to reward circuitry alleviates anhedonia in refractory major depression. Chapter 3 Novel therapeutic targets for major depressive disorder Marcio Gerhardt Soeiro-de-Souza and Rodrigo Machado-Vieira 3. This heterogeneous and chronic disorder is associated with frequent episode relapses and recurrences. Thus, the development of new, effective, and better-tolerated therapeutic approaches with a more rapid onset of action is critical. To achieve this objective, a variety of compounds targeting diverse new systems have been proposed and have been or are being tested. Many of these may ultimately result in new and improved treatments for mood disorders. Three types of opioid receptors have been described in the pathophysiology of mood disorders: delta, mu, and kappa. Notably, opioid receptors are co-expressed in brain areas implicated in the pathophysiology of mood disorders (Preskorn et al. For instance, patients with depression and anxiety were found to have lower serum -endorphin levels (Darko et al. In addition, antidepressants have been shown to reverse stress-related changes in dynorphin levels in diverse limbic brain areas (Chaki et al. Blocks voltage-gated sodium channels, thereby blocking glutamate release and enhancing astrocytic uptake of glutamate. Epigenetic changes can permanently alter gene expression, which may induce subsequent changes in behaviour; however, such effects may be potentially reversible over time (Kato et al. Histone acetylation has been considered a promising therapeutic target in mood disorders because of its ability to control epigenetic effects that regulate cognitive and behavioural processes. Supersensitivity to melatonin suppression by light was described in individuals with mood disorders and their unaffected offspring (Herken et al.
Multistage ethanol sclerotherapy of soft tissue arteriovenous malformations: effect on pulmonary arterial pressure treatment with cold medical term generic prochlorperazine 5 mg on-line. Transarterial embolization and ablation of renal arteriovenous malformation;efficacy and damages in 30 patients with long-term followup the treatment 2014 online prochlorperazine 5 mg without a prescription. Vena cava filter scaffold to prevent migration of embolic materials in the treatment of a massive renal arteriovenous malformation my medicine prochlorperazine 5 mg buy low cost. Conclusion Congenital vascular malformations are challenging management problems symptoms of strep buy genuine prochlorperazine online, and the interventionalist often has more to offer in terms of treatment than any other specialist medications after stroke discount prochlorperazine 5 mg with mastercard. Most lesions are treated on an elective basis but acute events such as bleeding, ischemia, and high-output cardiac failure may require urgent intervention. Proper diagnosis and a long-term view of the natural history of the condition, as well as a careful risk/ benefit analysis, are essential to achieving an optimal result. High-flow lesions are best managed by transcatheter embolization with the goal of reducing or eradicating the central nidus of the lesion. Proximal ligation or embolization should be avoided, as any benefit will be temporary and future intervention becomes more difficult. Venous malformations are best managed by direct injection sclerotherapy, often in staged procedures. Care must be taken in the choice of embolic agent, total dose used, and avoidance of systemic and local complications. While many malformations cannot be completely eradicated, clinical signs and symptoms can be markedly improved in the majority of patients. Endovascular radiofrequency ablation: a novel treatment of venous insufficiency in KlippelÂTrenaunay patients. Ethanol sclerotherapy of venous malformations: evaluation of systemic ethanol contamination. Superselective arterial embolization for the treatment of lower gastrointestinal hemorrhage. Endovascular treatment combined with emboloscleorotherapy for pelvic arteriovenous malformation. Curative treatment of pelvic arteriovenous malformation  an alternative strategy:transvenous intra-operative embolisation. Pelvic arteriovenous malformation treated by superselective transcatheter venous and arterial embolization. Transcatheter embolization of uterine arteriovenous malformation: report of 2 cases and review of literature. Uterine arteriovenous malformation successfully embolized with a liquid polymer, isobutyl 2-cyanoacrylate. In spite of the similar anatomical location of the pathophysiology in both acute and chronic forms of mesenteric ischemia, the difference in their clinical presentation and management mandate separate consideration of these conditions. Sudden onset of generalized abdominal pain with preexisting symptoms of chronic mesenteric ischemia may suggest acute thrombosis of advanced atherosclerotic lesions in the mesenteric vasculature. Other predisposing conditions include valvular heart diseases, left ventricular aneurysm, extensive atherosclerotic aortic disease, aortic dissection, and complications of aortic surgery. High clinical suspicion is the key as diagnosis is often missed due to nonspecific clinical findings. Abdominal pain is of sudden onset and severe but is generally not localized early on. Localization of this pain with peritoneal signs suggests transmural necrosis of bowel. Physical examination is usually unremarkable with occasional abdominal distension and diarrhea, which may become bloody as time progresses secondary to mucosal sloughing. Thrombolysis, both pharmacological and mechanical, has been successfully employed in only a few cases of very early diagnosis [11, 12]. The time required for complete lysis may not always be available as the window for restoring the blood flow is limited and the risk for distal embolization is high. Acute stenting, as employed in the coronary circulation, is generally not applicable in this setting. The patient may be so ill that diagnosis is delayed until it is too late for treatment. The patient is generally in a low-flow state secondary to cardiogenic shock or septic shock and is often on a high-dose vasopressor agent. A high index of suspicion in any patient who develops abdominal pain in the suggested clinical settings leads to the diagnosis which is most often confirmed by contrast angiography. Plain abdominal radiograph (A) demonstrates effacement of normal small bowel mucosal pattern with "thumbprinting" caused by mucosal edema, an early finding. Systemic anticoagulation with bowel rest and parenteral nutrition is the treatment of choice ChApter 49 Interventions for Mesenteric Ischemia 445 for patients without peritonitis. Compared with systemic anticoagulation, early mechanical or pharmacological thrombolysis of acute portomesenteric venous thrombosis via a transjugular or percutaneous transhepatic approach prevents progression of bowel ischemia in the short term and in the long term prevents development of portal hypertension [22]. Surgical repair of the proximal intimal tear is the most effective treatment for type A dissection [23]. Endovascular treatment of acute complicated type B dissection with malperfusion syndrome has a low morbidity and mortality compared to open repair and may now be considered the therapy of choice [23Â25]. In some cases of aortic dissection, distal reperfusion may involve stenting of the visceral branches and endovascular fenestration of the aortic septum. Percutaneous fenestration can be achieved with either a reentry needle or the stiff end of the 0. Open surgical approach to malperfusion syndrome is by resection of the dissecting septum with direct repair of the ostia of visceral vessels. Vasculitis affecting small and medium size vessels is a rare cause of mesenteric ischemia [26]. Takayasu disease may affect the visceral aorta and cause narrowing of major branches with eventual fibrosis and scarring which can lead to thrombosis and extensive mesenteric ischemia. A balloon fenestration may be performed to equalize the pressure in the false and true lumens (B). The typical presentation consists of postprandial abdominal pain, progressing to "food fear" and eventually leading to weight loss, which is often dramatic [4]. Occlusion or stenosis of the celiac trunk is actually fairly common, due to either atherosclerosis or extrinsic compression by the arcuate ligament of the diaphragm (median arcuate ligament syndrome, discussed below). Aside from the history and obvious cachexia, there are few specific clinical findings to suggest the diagnosis. Abdominal bruits, while considered a classic physical finding, are often appreciated retrospectively after the diagnosis has been made. Color flow Doppler imaging is now being used increasingly as a cost-effective and noninvasive modality to diagnose mesenteric arterial stenosis. Currently, catheter angiography is performed primarily to confirm the diagnosis, allow treatment planning, and in selected cases to carry out endovascular intervention. Some believe that symptoms associated with arcuate ligament compression are actually related to compression of the celiac ganglion which lies on top of the artery. This could be a proximal atherosclerotic lesion (note calcification) but may also represent arcuate ligament compression. The involvement resembles that found in the renal artery in that the process is an extension of the aortic wall disease into the ostium of the vessel. This localized nature of the disease makes it suitable for both surgical and endovascular treatments. The choice of treatment is somewhat controversial at present, with each approach having strong advocates. Late follow-up in one of the largest case series reported a 76% freedom from symptoms in those treated with both celiac decompression and revascularization versus only 53% in those treated with decompression alone [32]. Traditionally, open surgical repair has been the standard for chronic mesenteric ischemia. Open revascularizations are durable with a 81Â92% symptom-free survival at 3Â5-year follow-up [37Â41]. The disadvantages of open repair are higher morbidity (20Â30%) and mortality (4Â15%) with prolonged hospitalization [37Â39, 41]. However, a few others have noted similar mortality but higher morbidity with open repair [38]. In a recent review of such retrospective studies comparing open versus endovascular repair [40], overall results were comparable between the two modes of treatment in terms of technical success (100% versus 95%) and immediate pain relief (93% versus 88%). Endovascular repair has the advantage of decreased short-term morbidity but the disadvantage of decreased long-term primary patency compared with open repair in several series: 58% versus 90% at 1 year [44], 27% versus 66% at 3 years [13], and 41% versus 88% at 5 years [38]. She developed restenosis due to progression of the ostial disease, as the initial stent was placed slightly too distally (C). Open repair, on the other hand, has excellent durability and should be considered the best treatment for a patient fit for surgery and with lesions not amenable to endovascular repair. ChApter 49 Interventions for Mesenteric Ischemia 451 endovascular technique and stent selection Once the diagnosis of acute visceral ischemia is suspected, abdominal angiography should be performed on an emergent basis. The superior mesenteric artery is by far the most critical of the three visceral trunks and due to its size and anatomical alignment with the aorta, it is the vessel most frequently involved by embolus. Starting with selective catheterizations risks showering proximal emboli distally, which might turn a simple embolectomy into a case of multiple distal occlusions, which cannot be salvaged. Even in the presence of an acute embolic occlusion, angiography will nearly always demonstrate some distal reconstitution of mesenteric branches. In general, if the patient is an operative candidate operative embolectomy should be carried out immediately and the viability of the bowel can be assessed at the same time. If, however, a lesion is deemed amenable to endovascular treatment, the short sheath is then replaced by a long sheath. The diseased segment of the artery is crossed with a steerable but atraumatic wire which is then exchanged for a more supportive wire which will enable balloon and stent placement. In terms of stent selection, precise placement and superior radial strength have favored the use of balloon-expandable rather than self-expanding stents in the visceral circulation. Since these are generally ostial lesions, it is important to extend the stent slightly into the aortic lumen in order to prevent plaque progression and stent occlusion. Embolic protection devices have been recommended by some authors but are not at present used in most institutions performing visceral stenting. They are somewhat problematic to use in ostial lesions, and if they are positioned in the hepatic artery there is a risk of spasm or dissection of this unusually delicate vessel. Some authors routinely use an upper extremity approach (radial, brachial, axillary) for visceral stenting due to the acute angle of take-off of the visceral trunks. In our institution, we generally start with a femoral approach, which provides more catheter control and shorter systems. The authors noted no difference in the patency rates irrespective of the stent type, size, number or the vessel treated. Less angulation is present when working from a brachial approach, but it is more cumbersome and longer delivery systems are needed. Single vessel versus multiple vessel intervention and recurrent disease Controversy persists over whether a single vessel intervention is better than multivessel treatment. While a few studies [37, 41] have shown equivalent outcomes after single and multiple vessel revascularization, the better long-term patency and symptom-free survival of open revascularization has been attributed to a multivessel intervention. Similar differences have been observed in other studies [13] with a proposal to improve durability of endovascular treatment by two-vessel revascularization. Although duplex ultrasound is not as accurate in stented vessels as in native arteries, it does offer an inexpensive and easily available noninvasive objective tool with which to follow these patients. At our institution we routinely study patients with duplex ultrasound at 1-month, 3-month, and 6-month intervals. Hence patient education is of paramount importance and they are explicitly instructed to seek urgent medical care if they experience any abdominal symptoms. Use of an embolic protection device was recommended for high-risk lesions mentioned above [57]. Antiplatelet therapy started before the procedure also decreased the risk of embolization and thrombosis. During attempted subselective catheterization the superior mesenteric artery was acutely dissected (B). Emergency stenting was performed from a brachial approach using a self-expanding stent (C). Conclusion Mesenteric ischemia is a relatively uncommon condition but one in which delayed diagnosis and intervention can be deadly. Acute mesenteric ischemia is an extreme emergency, as delayed diagnosis and treatment will rapidly lead to intestinal infarction and high mortality. The most common cause of acute mesenteric ischemia is embolization from a cardiac source, while less commonly it may occur in the setting of acute thrombosis ChApter 49 Interventions for Mesenteric Ischemia 455 of a chronic atherosclerotic lesion, acute aortic dissection, or iatrogenically. Most embolic occlusions are handled surgically, as the window for restoration of mesenteric flow is short and embolectomy is a fairly straightforward undertaking. There has been an increasing use of endovascular techniques, but their role in the acute setting remains unclear. Chronic mesenteric ischemia can present insidiously, and its manifestations frequently mimic other abdominal conditions so that diagnosis is often delayed. The hallmarks of the condition include postprandial pain, weight loss, and "food fear," and it is generally encountered in patients with known widespread atherosclerotic disease. The optimal type of intervention remains controversial, with advocates of both endovascular and open surgical revascularization. Stenting can be performed safely with minimal morbidity but open surgical reconstruction has indisputably better long-term patency, at least at present. Determinants of mortality and treatment outcome following surgical interventions for acute mesenteric ischemia. Contemporary management of acute mesenteric ischemia: factors associated with survival. A comparison of endovascular revascularization with traditional therapy for the treatment of acute mesenteric ischemia.
Other adjuvants In 1987 treatment solutions prochlorperazine 5 mg buy on line, a single case report described the development of discoid lupus erythematosus in a smallpox vaccination scar; however treatment spinal stenosis discount prochlorperazine 5 mg overnight delivery, no other cases have been reported in the literature since medicine norco buy prochlorperazine 5 mg otc, probably due to the uncommon use of the smallpox vaccination in the general population (Lupton treatment management company order prochlorperazine with mastercard, 1987) symptoms 10dpo 5 mg prochlorperazine order with visa. Influenza virus vaccination of patients with systemic lupus erythematosus: effects on disease activity. Influenza vaccination of patients with systemic lupus erythematosus: safety and immunogenicity issues. Early clinical manifestations in a large cohort of patients with undifferentiated connective tissue diseases compared with cohorts of well-established connective tissue disease. Influenza vaccine administration in patients with systemic lupus erythematosus and rheumatoid arthritis: safety and immunogenicity. Stress hormones, Th1/Th2 patterns, pro/anti-inflammatory cytokines and susceptibility to disease. The sympathetic nerveÂan integrative interface between two supersystems: the brain and the immune system. Immunogenicity and safety of pneumococcal vaccination in patients with rheumatoid arthritis or systemic lupus erythematosus. Pneumococcal vaccination of patients with systemic lupus erythematosus: effects on generation of autoantibodies. A caseÂcontrol study of serious autoimmune adverse events following hepatitis B immunization. Influence of microbial stimulation on hypergammaglobulinemia and autoantibody production in pristane-induced lupus. The sick building syndrome as a part of the autoimmune (autoinflammatory) syndrome induced by adjuvants. Alum adjuvant boosts adaptive immunity by inducing uric acid and activating inflammatory dendritic cells. Prevalence of human papilloma virus infections and cervical cytological abnormalities among Korean women with systemic lupus erythematosus. Nephritogenic autoantibodies in lupus: current concepts and continuing controversies. Pneumococcal immunization in patients with systemic lupus erythematosus treated with immunosuppressives. Clinical and antibody responses after influenza immunization in systemic lupus erythematosus. Prevalence of cervical human papillomavirus infection in women with systemic lupus erythematosus. Anti-tetanus toxoid antibody synthesis after booster immunization in systemic lupus erythematosus. Virus antibodies in systemic lupus erythematosus and other connective tissue diseases. Autoimmune response following influenza vaccination in patients with autoimmune inflammatory rheumatic disease. Cervical human papillomavirus infection in Mexican women with systemic lupus erythematosus or rheumatoid arthritis. The occurrence, pathogenesis and significance of autoimmune manifestations after viral vaccines. Autoimmune (autoinflammatory) syndrome induced by adjuvants provides a diagnostic framework for enigmatic conditions. Analysis of costimulatory molecule expression on antigen-specific T and B cells during the induction of adjuvant-induced Th1 and Th2 type responses. No short-term immunological effects of Pneumococcus vaccination in patients with systemic lupus erythematosus. Mechanisms of aluminum adjuvant toxicity and autoimmunity in pediatric populations. Autoimmune response following annual influenza vaccination in 92 apparently healthy adults. Autoantibody response to adjuvant and nonadjuvant H1N1 vaccination in systemic lupus erythematosus. Clinical outcome and predictors of disease evolution in patients with incomplete lupus erythematosus. Influenza vaccination can induce new-onset anticardiolipins but not 2-glycoprotein-I antibodies among patients with systemic lupus erythematosus. They show different etiologies, pathogeneses, genetic predispositions, types of vessels affected, organ distributions, types of inflammation, clinical manifestations, and distinctive demographic characteristics; these and other features can be used for disease categorization (Jennette et al. In particular, the new system separates vasculitides with known causes  such as infections  from those without known causes. Several reports of vasculitis onset following exposure to vaccines have been described since the 1970s. Nevertheless, these phenomena remain rare, so it is difficult to establish whether some specific vaccines should be included among the environmental factors sometimes associated with the development of these diseases. As a matter of fact, to date a clear etiological definition of "post-vaccination" vasculitides is still missing. In this chapter, we discuss the main etiopathogenic hypotheses for how vasculitic processes may be triggered by vaccines, and we analyze all the relevant Medline records from 1970 through July 2013 relating to the onset of different types of vasculitides following exposure to different vaccines. Vasculitides following vaccinations: plausible mechanisms Vaccines contain viral or bacterial antigens, in many cases in combination with adjuvants and with several types of preservatives. As each component of a vaccine might induce blood vessels inflammation via several mechanisms, many plausible theories have been proposed for the etiopathogenic link between exposure to such stimuli and the onset of these diseases. The role of infectious agents In recent decades, it has become clear that infectious agents and vaccines have many similarities Vaccines and Autoimmunity, First Edition. Manna in their ability to facilitate antibody production, immune reactions, and a wide spectrum of autoimmune phenomena, including vasculitides (Kivity et al. This overlapping of vaccine/infection-induced immune responses is not a surprising feature, given that the essence of a vaccine is, in many cases, a live-attenuated or recombinant pathogenic antigen (Chen et al. For others, animal models provide additional validity to the hypothesis of such a link (Mathieson et al. Several mechanisms are thought to be involved in the pathogenesis of infection-related vasculitides, among which are direct microbial invasion of vessel wall endothelial cells, vessel wall damage induced by immune complex formation, and B and T cell stimulation through molecular mimicry and superantigens. In some cases, more than one mechanism is involved (Millikan and Flynn, 1999; Guillevin, 2004; Rodriguez-Pla and Stone, 2006; Lidar et al. Vaccines may provide a transient inflammatory setting for bystander activation and autoreactive T cells through antigen nonspecific mechanisms, which can initiate the autoimmunity process. Additional viral infections have been found to have an association with vasculitic syndromes. However, in recent years, many adjuvants have been found to trigger autoimmunity themselves (Gherardi and Authier, 2003; Satoh et al. Such adjuvants merge the diverse and multifaced autoimmune and inflammatory reactions caused by different pharmaceutical, industrial, and environmental compounds with the immune-mediating capabilities of an "adjuvant effect" (Shoenfeld and Agmon-Levin, 2011). All of these are vectors used in vaccine preparation, manufacturing, and preservation. In particular, immediate hypersensitivity reactions are generally considered to be transient post-vaccination phenomena, and they have been related to hypersensitivity to injected foreign antigens. Delayed reactions include urticarial vasculitides, neutrophilic dermatoses, and maculopapular exanthems. All of the post-vaccination syndromes, including systemic post-vaccine vasculitides, appear to have surprising similarities in their signs and symptoms to the usual "pattern" of disease presentation. Nevertheless, they may contain thimerosal: in the formulation of multidose vials, it is used as a preservative to prevent bacterial overgrowth, and it may trigger the inflammatory response in susceptible subjects. Clinical evidence from the literature We performed a Medline search of all relevant publications, without any date limitation, and with special emphasis on finding each kind of vasculitide linked to exposure to different types of vaccines. Medium-vessel vasculitides the first case of medium-vessel vasculitis related to vaccine exposure was described in 1983 by Guillevin et al. It is the second most frequently administered vaccine in the United States (Zhou et al. Despite the fact it has been declared "generally well tolerated," few large series on serious autoimmune adverse events have been reported (Grotto et al. The time interval between vaccine administration and onset of clinical manifestations varied from 1 day to 3 months. As seen with infectious agents, an immune complex may form between vaccine antigens and native antibodies, thereby initiating the vasculitic process. Mastroiacovo (1976) described the first case following smallpox vaccine in 1976, hypothesizing a causal relationship between vaccines and rheumatic disorders in the pediatric population for the first time. The most commonly reported symptoms include arthralgias, rashes, joint swelling, abdominal pain, and proteinuria. The reported time course of symptom onset after vaccine administration ranges from a few hours to 14 days. However, where there is a short delay between vaccine administration and onset of clinical manifestations, the hypothesis of a hypersensitivity reaction to the vaccine or to any of its adjuvants and preservatives should be considered. An abnormal activation of the immune system and a direct effect of the vaccine itself, involving triggering of autoreactive T cells or a deregulated cytokine network, have been described as possible mechanisms. The final result is the deposition of immune complexes at the vessels, which is the pathophysiologic hallmark of leukocytoclastic vasculitides. In other cases, they can result from hypersensitivity to some components of the vaccine. Conclusions Because the incidence of post-vaccination vasculitides remains very low, vaccinations should not be limited for this reason. Some authors suggest that children with a history of vaccine-induced vasculitides should not be revaccinated, but there are currently no clear guidelines for what is the most appropriate management. It has been suggested that flu vaccines must be contraindicated in subjects with a history of rheumatoid purpura, with previous history of vasculitis after flu vaccination, or with active autoimmune rheumatic disease. Further investigations are needed to clarify the biologic plausibility of post-vaccination phenomena. Thus, surveillance systems and registries can be important tools for retrospective as well as prospective evaluations of cases, and also for establishing research studies aimed at elucidating genetic susceptibility factors. Nevertheless, in clinical practice, when the suspicion of vasculitis onset is raised, a meticulous history-taking with special emphasis on vaccine history is imperative, so that an appropriate diagnosis can be established early and management can be initiated. Moreover, follow-up is mandatory to verify whether a different prognosis is associated with these diseases. The lack of evidence for other causes of the symptoms and the coincidence regarding the vaccination in most of the cases analyzed here strongly supports a causal relationship between the vaccination and vasculitis onset, especially where a plausible temporal association exists. For this reason, the modal peak in time of the onset has to be carefully examined, in order to detect cases with peak onset within a few days of vaccination (which are more consistent with hypersensitivity reactions) or within weeks or months (which are more consistent with delayed immune reactivity). Infection of endothelial cells with virulent Rickettsia prowazekii increases the transmigration of leukocytes. Infection of human vascular endothelial cells with Staphylococcus aureus induces hyperadhesiveness for human monocytes and granulocytes. Churg-Strauss vasculitis with brain involvement following hepatitis B vaccination. Bacterial induction of autoantibodies to beta2 glycoprotein-I accounts for the infectious etiology of antiphospholipid syndrome. Streptococcal and staphylococcal superantigen -induced lymphocytic arteritis in a local type experimental model: comparison with acute vasculitis in the Arthus reaction. Chronic fatigue syndrome with autoantibodies-the result of an augmented adjuvant effect of hepatitis-B vaccine and silicone implant. Progression of renal disease in Henoch-Schцnlein purpura after influenza vaccination. Antineutrophil cytoplasmic antibody vasculitis associated with influenza vaccination. Chronic parvovirus B19 infection and systemic necrotising vasculitis: opportunistic infection or aetiological agent? Aggravation of anti myeloperoxidase antibody-induced glomerulonephritis by bacterial lipopolysaccharide: role of tumor necrosis factor alpha. Necrotizing glomerulonephritis in decursu vasculitis after vaccination against influenza. Thrombocytopenic purpura after measles, mumps and rubella vaccination: a retrospective survey by the French regional pharmacovigilance centres and Pasteur-Mйrieux sйrums et vaccins. Case of mycroscopic polyangiitis and giant cell arteritis after influenza vaccination. Dapsone in allergic vasculitis: its use in Henoch-Schцnlein disease following vaccination. Hypersensitivity reactions to vaccine constituents: a case series and review of the literature. Systemic vasculitis following influenza vaccination  report of three cases and literature review. Infection of human endothelial cells with Staphylococcus aureus induces transcription of genes encoding an innate immunity response. Lymphocytic vasculitis associated with the anthrax vaccine: case report and review of anthrax vaccination. A clinical analysis of gelatin allergy and determination of its causal relationship to the previous administration of gelatin containing acellular pertussis vaccine combined with diphtheria and tetanus toxoids. Hepatitis B vaccination and central nervous system demyelination: an immunological approach. Aluminum hydroxide injections lead to motor deficits and motor neuron degeneration. Giant cell arteritis and polymyalgia rheumatica after influenza vaccination: report of 10 cases and review of the literature. Vaccination of healthy subjects and autoantibodies: from mice through dogs to humans. Giant cell arteritis with polymyalgia rheumatica associated with influenza vaccination.
Purchase generic prochlorperazine on-line. How to fill out a supplemental anxiety questionnaire form SSA and DDS.
References
- Pillai J, Levien LJ, Haagensen M, et al: Assessment of the medial head of the gastrocnemius muscle in functional compression of the popliteal artery, J Vasc Surg 48:1189-1196, 2008.
- Bishop CV, Liddell H, Ischia J, et al: Holmium laser enucleation of the prostate: comparison of immediate postoperative outcomes in patients with and without antithrombotic therapy, Curr Urol 7(1):28n33, 2013.
- Afzelius BA. Cilia-related diseases. J Pathol 2004;204:470-7.
- Rubbia-Brandt L, Audard V, Sartoretti P, et al. Severe hepatic sinusoidal obstruction associated with oxaliplatin-based chemotherapy in patients with metastatic colorectal cancer. Ann Oncol. 2004;15(3):460-466.
- Chamberlain MC. Should erlotinib be coadministered with whole-brain radiotherapy in patients with brain metastases and non-small-cell lung cancer? J Clin Oncol 2013; 31(25):3164-3165.
- Kreuning P, Bosman FT, Kuiper G, van der Wal AM, Lindeman J. Gastric and duodenal mucosa in 'healthy' individuals. An endoscopic and histopathological study of 50 volunteers. J Clin Pathol 1978;31:69.