- info@careermakers.edu.np
- +977 1 4423870
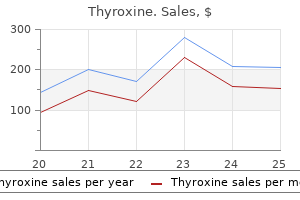
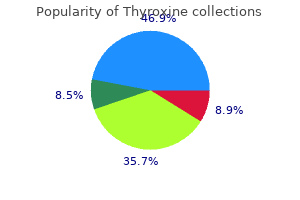
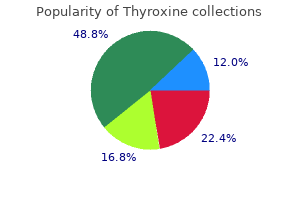
Thyroxine

Jenny K Hoang, M.B.A., M.B.B.S., M.H.S.
- Vice Chair of Radiology Enterprise Integration
- Associate Professor of Radiology and Radiological Science
https://www.hopkinsmedicine.org/profiles/results/directory/profile/10004927/jenny-hoang
Glucocorticoid inhibition of growth in rats: Partial reversal with somatostatin antibodies medicine prices cheap thyroxine 125 mcg without a prescription. Cyclosporin-A in vivo produces severe osteopenia in the rat: Effect of dose and duration of administration symptoms xanax withdrawal buy thyroxine 25 mcg amex. Azathioprine alone is bone sparing and does not alter cyclosporin A-induced osteopenia in the rat treatment uterine fibroids discount 200 mcg thyroxine amex. Recombinant human growth hormone treatment of children following renal transplantation medications prescribed for migraines order thyroxine cheap online. Early subclinical coronary artery calcification in young adults who were pediatric kidney transplant recipients treatment enlarged prostate thyroxine 50 mcg buy visa. Elevated fibroblast growth factor 23 is a risk factor for kidney transplant loss and mortality. On examination, he is found to be a pale boy with a height and a weight that are both below the 3rd percentile. An 8-year-old girl presents with reflux nephropathy and growth failure and has the following serum biochemical determinations: Serum creatinine, 2. A 10-year-old boy receiving maintenance hemodialysis is treated with calcium carbonate and thrice weekly calcitriol to control his renal osteodystrophy. The nutritional status and requirements for these patients need to be evaluated regularly with the goals of maintaining a normal pattern of growth and body composition and avoiding electrolyte abnormalities, uremic toxicity, and malnutrition. Length can be measured using a length board, and height using a wall-mounted stadiometer. Therefore, a careful clinical examination is warranted, and indicators of volume status including edema, hypertension, pulse rate, skin turgor, or laboratory indices such as sodium or albumin levels, must be evaluated. The height-for-age percentiles must be taken into account when looking at the weight-for-age percentiles. Children who depend solely on enteral feeding may benefit from more frequent monitoring. The dietary intake should be assessed with either a prospective 3-day diet diary or three 24-hour diet recalls. Information obtained from either method can then be used by a registered dietitian to estimate the daily intake of energy, macronutrients, vitamins, and minerals and overall dietary adequacy. Further studies are needed to validate this new methodology and to justify its clinical utility. Patients on chronic peritoneal dialysis lose significant amounts of protein through the dialysate, with infants on peritoneal dialysis having almost twofold more peritoneal protein loss per body surface area (m2) compared to older children weighing more than 50 kg. Ghrelin is an orexigenic hormone with additional effects on the regulation of inflammation and the cardiovascular system. There are three circulating Nutritional management in chronic kidney disease / Energy 669 products of the ghrelin gene: acyl ghrelin, des-acyl ghrelin, and obestatin, each with individual distinct functions on appetite regulation. Leptin is an anorexigenic hormone that is secreted from the adipocytes and interacts with ghrelin and other appetite-regulating hormones. Leptin also plays a role in regulating inflammation and the cardiovascular system. Low vitamin D levels upregulate the renin-angiotensin-aldosterone system, increase inflammation, and cause endothelial dysfunction. Epidemiologic studies suggest an association between low vitamin D levels and risk factors for cardiovascular disease, but a causal relationship has not been established. For example, infants with low birth weight and patients with recurrent vomiting may require supplemental calories to maintain growth. On the other hand, patients on peritoneal dialysis who demonstrate excessive weight gain may need reduction of their energy intake to take into account the energy intake from dialysate glucose, which is estimated at 8 to 12 kcal/ kg/day. The development of such a program requires a team approach in which the role of the dietitian is vital. Several components have to be considered in developing the dietary prescription, including energy, macronutrients, micronutrients, fluid, and electrolytes. In a study of European children on chronic dialysis, overweight and obesity, rather than underweight, were highly prevalent. Short stature among kidney allograft recipients strongly correlated with overweight, whereas underweight appeared to be a problem only in infants. These findings suggest that nutritional management in children receiving chronic dialysis should focus as much on the prevention and treatment of overweight as on preventing cachexia and protein energy wasting. Poor oral intake, recurrent emesis, and poor weight gain and growth should prompt initiation of tube feedings. Tube feedings can relieve the stress that comes with trying to meet nutritional requirements34 and have a low complication rate. For children older than 3 years of age, calories from carbohydrates should make up 45% to 65%, fat 25% to 35%, and protein 10% to 30% of total intake. For children 1 to 3 years of age, the distribution of calories from carbohydrate, fat, and protein should be 45% to 65%, 30% to 40%, and 5% to 20% of total caloric intake, respectively (see Table 34. Therefore, the distribution of carbohydrate, fat, and protein should be consistent with infant formula, which is 36% to 56% carbohydrate, 40% to 54% fat, and 7% to 12% protein. The protein requirements for these children may vary depending on various clinical conditions such as proteinuria and catabolism. Because patients on peritoneal dialysis experience loss of protein through the dialysate ultrafiltrate that is inversely related to body weight and peritoneal surface area and protein supplementation differs according to the patient age and ranges from 0. Infants, who have a larger peritoneal surface area than older children, will therefore require more protein supplementation on a Gram-per-kilogram basis. However, studies in both adults41,42 and children43,44 showed no benefit with lowprotein diets, with some studies actually indicating potential adverse effects of a diet very low in protein, including Nutritional management in chronic kidney disease / Fat 671 relatively low in phosphorus should be selected when possible. Protein derived from animal flesh contains the lowest amount of phosphorus (11 mg of phosphorus per 1 g of protein), whereas protein derived from plants (legumes and lentils), eggs, or dairy products contains higher amounts of phosphorus (20 mg of phosphorus per 1 g of protein). Therefore, dietary protein that is not entirely derived from animal products and that also contains vegetable sources of protein is recommended. Simple sugars should be restricted to avoid hypertriglyceridemia, especially in the early post-transplant period when there is a higher risk for developing glucose intolerance and hyperglycemia from corticosteroid and calcineurin inhibitor therapy. Dietary fiber, which is found in most vegetables, fruits, and whole grains, can help reduce cholesterol levels and therefore decrease the risk for cardiovascular disease. Children on strict fluid restrictions may be limited in the amount of fiber they can consume because of the water intake required with such a diet. Heart-healthy fats such as oils produced from plant sources such as canola, corn, soybean, and olives are recommended. These dietary changes should be implemented in conjunction with controlling caloric intake and increasing physical activity. The beneficial effects of omega-3 fatty acids on cardiovascular disease and prevention have been widely studied in adults. Omega-3 fatty acids have been reported to reduce serum triglyceride levels, blood pressure, thrombotic risk factors, and inflammation in adult patients. In a small study of 16 children (7 to 8 years of age) on dialysis, 8 weeks of daily oral fish oil supplementation (3 to 8 g/day) resulted in a 27. The kidneys are responsible for excreting excess phosphorus and converting 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D, the active form of vitamin D. As renal function declines, hyperphosphatemia and hypocalcemia develop, eventually leading to renal osteodystrophy. Target level of calcium and phosphorus are age-based because normal levels of calcium and phosphorus are higher in younger age groups. Alternative medications that have less of a hypercalcemic effect are now available, including less calcemic active vitamin D analogues. If available, a liquid containing the B vitamins and vitamin C can be used for infants and children unable to swallow tablets. If the liquid form is not available, an adult renal supplement containing the B vitamins and vitamin C can be crushed and dissolved in water. Infants and toddlers are usually given half a tablet and older children are given 1 tablet daily. Nutritional management in chronic kidney disease / Calcium, Phosphorus, and Vitamin D 673 Table 34. Adverse clinical outcomes associated with short stature at dialysis initiation: A report of the North American Pediatric Renal Transplant Cooperative Study. European Study Group for Nutritional Treatment of Chronic Renal Failure in Childhood. Growth impairment shows an age-dependent pattern in boys with chronic kidney disease. Neurodevelopmental outcome of children initiating peritoneal dialysis in early infancy. Normalized protein catabolic rate versus serum albumin as a nutrition status marker in pediatric patients receiving hemodialysis. Models to assess nitrogen losses in pediatric patients on chronic peritoneal dialysis. Simple nutritional indicators as independent predictors of mortality in hemodialysis patients. Hypoalbuminemia and risk of death in pediatric patients with end-stage renal disease. Changes in bone structure and the muscle-bone unit in children with chronic kidney disease. Longterm enteral nutrition in infants and young children with chronic renal failure. Dietary prescription based on estimated nitrogen balance during peritoneal dialysis. Nutritional status of children undergoing continuous ambulatory peritoneal dialysis. Conservative treatment for chronic renal failure from birth: A 3-year follow-up study. Underweight, overweight and obesity in paediatric dialysis and renal transplant patients. Feeding dysfunction in infants with severe chronic renal failure after long-term nasogastric tube feeding. Growth posttransplantation in children previously treated with chronic dialysis and gastrostomy feeding. Intradialytic parenteral nutrition in malnourished children treated with hemodialysis. Intradialytic parenteral nutrition treatment and biochemical marker assessment for malnutrition in adolescent maintenance hemodialysis patients. Effect of dietary protein restriction on nutritional status in the Modification of Diet in Renal Disease Study. Randomised multicentre study of a low-protein diet on the progression of chronic renal failure in children. European Study Group of Nutritional Treatment of Chronic Renal Failure in Childhood. Regression equation predicts dietary phosphorus intake from estimate of dietary protein intake. Phosphorus homeostasis in normal health and in chronic kidney disease patients with special emphasis on dietary phosphorus intake. Fiber, lipids, and coronary heart disease: A statement for healthcare professionals from the Nutrition Committee, American Heart Association. Cardiovascular risk reduction in high-risk pediatric patients: A scientific statement from the American Heart Association Expert Panel on Population and Prevention Science; the Councils on Cardiovascular Disease in the Young, Epidemiology and Prevention, Nutrition, Physical Activity and Metabolism, High Blood Pressure Research, Cardiovascular Nursing, and the Kidney in Heart Disease; and the Interdisciplinary Working Group on Quality of Care and Outcomes Research: Endorsed by the American Academy of Pediatrics. Progression in chronic kidney disease and prevention strategies [educational paper]. National Cholesterol Education Program: Report of the Expert Panel on Blood Cholesterol Levels in Children and Adolescents. Growth until 3 years of age in a prospective, randomized trial of a diet with reduced saturated fat and cholesterol. Omega-3 long-chain polyunsaturated fatty acids supplementation on inflammatory biomarkers: A systematic review of randomised clinical trials. Fish oil treatment of hyperlipidemia in children and adolescents receiving renal replacement therapy. Relationship between intact 1-84 parathyroid hormone and bone histomorphometric parameters in dialysis patients without aluminum toxicity. What parathyroid hormone levels should we aim for in children with stage 5 chronic kidney disease: What is the evidence No association has been found between low body mass index and increased risk for mortality in children. Rates of linear growth and neurodevelopment are highest during the second decade of life. The four circulating gene products of ghrelin include acyl ghrelin, des-acyl-ghrelin, obestatin, and melatonin. For children older than 3 years of age, which of the following distributions of calories from carbohydrates, fat, and protein is recommended Carbohydrates 45% to 65%, fat 25% to 35%, protein 10% to 30% Which of the following macronutrients is lost through the peritoneal dialysate ultrafiltrate Restricting dietary fat to 30% of the total caloric intake has adverse effects on growth. Which one of the following vitamin supplements is recommended in children on dialysis Since then, the technique introduced by Peter Kramer has evolved and has been modified further to provide both convective and diffusive exchange of solutes for enhanced solute clearance. To achieve predictable and controlled ultrafiltration, pump-assisted systems were developed in early 1990s and replaced arterial blood pressuredriven systems. These devices are a far cry from the simple and unconventional design envisioned by Peter Kramer. This is especially important in small children, who may require sedation for the procedure to be conducted safely.
Approximately 10% to 15% of plasma inorganic phosphorus is protein bound medications zoloft side effects 200 mcg thyroxine purchase with amex, and the remaining 85% to 90% is ultrafiltrable by the glomeruli symptoms joint pain fatigue generic thyroxine 200 mcg with amex. Whereas the adult phosphorus balance is zero medicine kim leoni buy cheap thyroxine 100 mcg, growing children have a positive phosphorus balance to meet the needs of skeletal growth symptoms 4 days before period quality thyroxine 100 mcg. Serum phosphorus is governed by a circadian rhythm symptoms wisdom teeth purchase thyroxine in india, with a rapid decrease in levels early in the morning, a nadir before noon, and a peak after midnight. When measuring the serum phosphorus level, it is best to obtain a specimen in the morning fasting state to minimize the effect of dietary changes on the serum level. The normal serum concentration of phosphorus varies with age, with values higher in infants than in older children and adults (Table 13. Other factors that may affect the serum level include metabolic acidosis and intravenous calcium infusion, both of which may increase the serum phosphorus. Decreased serum phosphorus levels may result from intravenous infusion of glucose or insulin, acute respiratory alkalosis, and epinephrine administration. Proximal tubular phosphate transport is mediated by the sodium-phosphate (Na-Pi) cotransporter present in the apical brush-border membrane. The Na-Pi cotransporter picks one phosphate ion along with three sodium ions and delivers these into the proximal tubular cells. Most of the ingested phosphorus is absorbed from the duodenum and jejunum, through passive diffusion by a paracellular pathway. When the luminal concentration is low, phosphorus may also be absorbed actively by a sodiumdependent transcellular process. Once in the extracellular fluid compartment, phosphorus exists in equilibrium with the bone and soft tissue pools. The net result of all these factors is an increase in serum phosphorus concentration, with relatively little change in the serum calcium. Serum phosphorus may not reflect total body phosphorus levels because it is predominantly an intracellular ion. Both primary and secondary hyperparathyroidism may result in phosphaturia and consequent hypophosphatemia. Nonselective urinary phosphate wasting, leading to hypophosphatemia, can be seen in numerous renal diseases, such as Fanconi syndrome, distal renal tubular acidosis, postobstructive diuresis, and the diuretic phase of acute tubular necrosis. Hypophosphatemia with reduced urinary phosphorus excretion may result from nutritional deficiency of phosphorus, malnutrition, impaired intestinal absorption from phosphorus-binding antacids, or intestinal disorders. Refeeding with a large carbohydrate load after prolonged malnutrition, as well as leukemic blast crisis, in which phosphate is incorporated into the proliferating cells, can lead to hypophosphatemia. Intracellular phosphorus shift may also result from infusion of glucose, fructose, lactate and amino acids, exogenous administration of insulin, glucagon, androgens, and -agonists. Symptoms may include anorexia, vomiting, paresthesias, myopathy, rickets, confusion, and seizures (Table 13. Life-threatening events, such as cardiac failure, ventricular arrhythmias, hypotension, red blood cell hemolysis, rhabdomyolysis, respiratory failure, and coma, may result from severe phosphorus deficits (less than 1. Improvements in growth have been noted with such therapy, but nephrocalcinosis can be a side effect. Patients can present either in early childhood (1 to 3 years) or in the adolescent and adult age groups. Adults presenting with this disorder do not have any skeletal deformities, but they may have short stature, bone pain, and fatigue, and pseudofractures or stress fractures may be seen on radiographs. Post-renal transplantation hypophosphatemia Hypophosphatemia that can persist for up to several months is commonly seen after renal transplantation. Idiopathic hypercalciuria Renal phosphate wasting and hypophosphatemia was reported in a small group of children with idiopathic hypercalciuria. Hungry bone syndrome Hungry bone syndrome refers to the transient phenomenon of hypocalcemia and hypophosphatemia seen due to increased avidity of bone for calcium and phosphorus after the resolution of long-standing primary or secondary hyperparathyroidism. Manifestations of hypophosphatemia as well as hypocalcemia can persist for weeks to several months. Oral supplemental calcium and vitamin 224 Disorders of mineral metabolism D therapy is needed for treatment of most patients with hungry bone syndrome. An occasional patient may require prolonged intravenous calcium supplementation and vitamin D to avoid life-threatening hypocalcemia. This index provides a theoretical lower limit of serum phosphorus below which all filtered phosphate would be reabsorbed. Bone radiography for evidence of osteoporosis and bone densitometry may also help in determining the impact of hypophosphatemia and phosphaturia on bone health. The fractional excretion of phosphate in normal children is 15% to 20%, and it is lower in growing infants. Milk and milk products are particularly high in phosphorus content, and their intake may be encouraged in such patients. Care should be taken not to provide calcium supplementation with meals because this may further exacerbate hypophosphatemia through binding of dietary phosphorus with calcium and thereby preventing its absorption. Intravenous phosphorus infusion therapy is generally reserved for patients with symptomatic hypophosphatemia or a serum phosphorus level lower than 1 mg/dL. It is important to remember that for every 1 mmol of phosphorus ordered as potassium phosphate, the patient will also receive approximately 1. Outer aspect of the vertical axis on right and the left side represents data in mass units (mg/100 mL). The phosphate infusions are formulated in normal saline- or dextrose-containing solutions and may be incorporated in the intravenous hyperalimentation. However, these infusions should not be mixed with calcium-containing solutions such as Ringer lactate, because of the risk of precipitation. Hypocalcemia, hypomagnesemia, and hyperphosphatemia can result following intravenous infusion of phosphate, and patients need close monitoring for these electrolyte abnormalities. Hyperkalemia and consequent cardiac toxicity can result from potassium phosphate infusion, even in patients with normal renal function. Acute elevations in phosphorus usually cause hypocalcemia, and patients can become symptomatic with paresthesias, tetany, seizures, or cardiac arrhythmias. Neutra-Phos K Cytolytic disorders Hyperphosphatemia is caused by a rapid release of intracellular phosphate during cellular breakdown; potassium and magnesium levels are also increased as a result of intracellular release. K-Phos Original K-Phos Neutral 150 mg/ capsule 250 mg/ tablet 0 13 mmol/ tablet Hyperphosphatemia / Management of hyperphosphatemia 227 Table 13. Decreased urinary phosphate excretion denotes either renal impairment or other disorders. In patients with severely impaired kidney function, dialysis may be the only feasible treatment, but the efficiency of hemodialysis and peritoneal dialysis in removal of phosphorus is limited. The kidney plays an important role in maintaining the homeostasis of all three ions. Advances in our understanding of the hormonal control, cellular actions, and molecular mechanisms of their handling by the kidneys have resulted in a better understanding of many enigmatic clinical disorders. Indeed, these findings may have significant pharmacotherapeutic applications, including addressing cardiovascular disease relating to aberrant mineral metabolism. Cellular calcium transport in renal epithelia: Measurement, mechanisms, and regulation. Localization of 25-hydroxyvitamin D3 1a-hydroxylase and 24-hydroxylase along the rat nephron. Bioavailability and biological efficacy of a new oral formulation of salmon calcitonin in healthy volunteers. Calcitonin is a major regulator for the expression of renal 25-hydroxyvitamin D3 -1a-hydroxylase gene in normocalcemic rats. A genetic etiology for DiGeorge syndrome: Consistent deletions and microdeletions of 22q11. Mutations in the Ca(2+)-sensing receptor gene cause autosomal dominant and sporadic hypoparathyroidism. Clinical and biological heterogeneity in pseudohypoparathyroidism syndrome: Results of a multicenter study. Functional hypoparathyroidism and parathyroid hormone endorgan resistance in human magnesium deficiency. Inactivating mutations in the 25-hydroxyvitamin D3-1-alpha-hydroxylase gene in patients with pseudovitamin Ddeficiency rickets. An unusual form of primary vitamin Dresistant rickets with hypocalcemia and autosomal dominant hereditary transmission: Hereditary pseudo-deficiency rickets. Point mutations in the human vitamin D receptor gene associated with hypocalcemic rickets. Longterm nocturnal calcium infusions can cure rickets and promote normal mineralization in hereditary resistance to 1,25-dihydroxyvitamin D. Familial benign hypercalcemia (hypocalciuric hypercalcemia): Clinical and pathogenetic studies in 21 families. Clustered inactivating mutations and benign polymorphisms of the calcium receptor gene in familial benign hypocalciuric hypercalcemia suggest receptor functional domains. Casting new light on the clinical spectrum of neonatal severe hyperparathyroidism. Neonatal severe hyperparathyroidism: Genotype/phenotype correlation and the use of pamidronate as rescue therapy. Risk of hypervitaminosis D from prolonged feeding of high vitamin D premature infant formula. Chronic hypercalcemia as the presenting feature of tuberculous peritonitis in a hemodialysis patient. Subcutaneous fat necrosis of the newborn: Hypercalcaemia with hepatic and atrial myocardial calcification. Hypercalcaemia of malignancy and basic research on mechanisms responsible for osteolytic and osteoblastic metastasis to bone. Elevations in circulating 1,25-dihydroxyvitamin D in three patients with lymphoma-associated hypercalcemia. Calcitriol production in hypercalcemic and normocalcemic patients with non-Hodgkin lymphoma. Clinical manifestations and molecular investigation of 50 patients with Williams syndrome in the Greek population. Committee on Genetics 2001 health care supervision for children with Williams syndrome. Maternal and infantile hypercalcemia caused by vitaminD-hydroxylase mutations and vitamin D intake. Inherited primary renal tubular hypokalemic alkalosis: A review of Gitelman and Bartter syndromes. Pathophysiology of functional mutations of the thiazide-sensitive Na-Cl cotransporter in Gitelman disease. Intrafamilial phenotype variability in patients with Gitelman syndrome having the same mutations in their thiazide-sensitive sodium/chloride cotransporter. Neonatal hypomagnesemia with selective malabsorption of magnesium: A clinical entity. Decreased bicarbonate threshold and renal magnesium wasting in a sibship with distal renal tubular acidosis. Novel paracellin-1 mutations in 25 families with familial hypomagnesemia with hypercalciuria and nephrocalcinosis. Regulation of serum 1, 25-dihydroxyvitamin D3 by calcium and phosphate in the rat. Familial tumoral calcinosis: From characterization of a rare phenotype to the pathogenesis of ectopic calcification. Hypophosphatemia: An evidence-based approach to its clinical consequences and management. Autosomal dominant hypophosphatemic rickets/osteomalacia: Clinical characterization of a novel renal phosphate wasting disorder. Elevated fibroblast growth factor 23 levels as a cause of early postrenal transplantation hypophosphatemia. Hungry bone syndrome: Still a challenge in the post-operative management of primary hyperparathyroidism: A systematic review of the literature. Calculation of renal tubular reabsorption of phosphate: the algorithm performs better than the nomogram. Severe hyperphosphatemia and hypocalcemic tetany after oral laxative administration in a 3-month-old infant. Studies of the mechanism by which phosphate infusion lowers serum calcium concentration. The pathophysiology of altered calcium metabolism in rhabdomyolysis-induced acute renal failure: Interactions of parathyroid hormone, 25-hydroxycholecalciferol, and 1,25-dihydroxycholecalciferol. Hyperphosphatemic familial tumoral calcinosis: Response to acetazolamide and postulated mechanisms. Severe vascular calcification and tumoral calcinosis in a family with hyperphosphatemia: A fibroblast growth factor 23 mutation identified by exome sequencing. Hyperphosphatemic familial tumoral calcinosis: Odontostomatologic management and pathological features. All of the following hormones have a net effect of reducing serum phosphorus values except: a. Hypophosphatemia in Fanconi syndrome leads to which of the following hormonal changes Which of the following segments of the kidney handle the majority of magnesium homeostasis A. Ionized calcium is the biologically active component of total body calcium and comprises: a. When calculating the fractional excretion of magnesium, the plasma magnesium must be multiplied by 0.
Formation of advanced glycation end products Glucose in diabetic patients reacts nonenzymatically with proteins symptoms of dehydration thyroxine 125 mcg buy lowest price, lipids 714x treatment for cancer buy thyroxine 125 mcg, and nucleic acids to form Schiff bases characterized by carbon-nitrogen double bonds symptoms xanax treats buy genuine thyroxine. Extending the follow-up data to age 40 years in these children showed that 25% patients eventually developed microalbuminuria medicine to induce labor 25 mcg thyroxine order visa. The action of insulin is mediated via insulin receptors present on the podocyte cell surface symptoms 3 dpo thyroxine 25 mcg buy with visa. Low-level proteinuria, below 30 mg/dL, is defined as microalbuminuria (also known as albuminuria), which can be detected by immunodiffusion or other laboratory techniques. Although a 24-hour urine collection is the most accurate method for quantifying microalbuminuria, timed urine collections are often difficult or inaccurate in children. Diagnostic reliability of spot urine albumin to creatinine ratio and its linear correlation with microalbuminuria in a 24 hour urine sample is well established. Microalbuminuria should be assayed in the first morning urine sample to avoid overestimation because of orthostatic proteinuria. These patients had diabetes mellitus, advanced proteinuria, and hypertension, and renal pathologic findings on autopsy demonstrated glomerulosclerosis. It is important to recognize that diabetic patients also can have nondiabetic renal disease, such as glomerulonephritis and tubulointerstitial nephritis. Care of these patients is best considered as a team of clinical providers, educators, nurses, and nutritionists. For the purpose of the classification, at least one convincing KimmelstielWilson lesion (as in panel [f]) needs to be present. This has been largely attributed to a better glycemic control in diabetic patients. This combination has been shown to have an additive effect in reducing proteinuria in some studies. Calcium channel blockers are also effective therapies in treating hypertension in diabetic patients and are neutral in their impact on glycemic control. A recent report about calcium channel blockers helping cell loss in the pancreas is interesting and may change the utility of calcium channel blockers in the management of hypertension in diabetes. In addition to pharmacotherapy, usual hypertension management strategies, such as lower salt intake, exercise, and caffeine avoidance should also be instituted in the management of hypertension in diabetics patients. A more meaningful alternative is to consider the waist-toheight ratio, which is normally at or just below 50%, but reaches between 50% and 60% and above with severe visceral adiposity. In the 2430 children reported in the Third National Health and Nutrition Examination Survey (1988 to 1994), overall MetS prevalence was 4%, but its prevalence in overweight children was 30%. Intestinal bacteria have been causally implicated in the inflammatory processes associated with obesity and insulin resistance by increasing gut permeability, permitting excessive microbial translocation. Adipocyte dysfunction leads to monocyte and macrophage infiltration in the location of ectopic hypertrophied adipocytes. Release of cytokines from these tissue sites leads to a state of ongoing inflammation and insulin resistance. Adipocyte-triggered systemic inflammation It is increasingly apparent that obesity triggers systemic inflammatory response and insulin resistance, both of which are present in MetS. Preadipocytes are phagocytic cells that resemble macrophages in both morphology and patterns of gene expression. The mechanism for insulin resistance during inflammation induced by obesity is believed to be a physiologic response to make glucose available for the metabolic needs of an activated immune system. Qualitative and quantitative nutrient features are important in microbial translocation of endotoxin across the intestinal barrier-the putative inflammatory root cause of insulin resistance and the MetS. Diets high in calorie content, such as refined starches, sugar, saturated and trans fats, and low in long-chain polyunsaturated omega fatty acids, natural antioxidants, and fiber from fruits and vegetables have been shown to promote inflammation and insulin resistance, and contribute to the development of the MetS. Metabolic syndrome / Renal pathologic findings in obesity-related glomerulopathy 543 vegetables, combined with a sedentary lifestyle, has been considered an important factor in the development of MetS and preventable cardiovascular deaths. These four substrates that are not regulated by insulin deliver metabolic intermediates to hepatic mitochondria and promote lipogenesis and the ectopic adipose storage-a feature characteristic of MetS. Others have also demonstrated glomerulomegaly in the renal biopsies of obese children and adults. Without sufficient adipose cells for fat storage, excess calories are shunted into ectopic and hypertrophied adipocytes. These hypertrophied adipocytes become dysfunctional, have inadequate vascular supply, and are at a heightened risk for apoptosis. Proteinuria, when present, is usually subnephrotic in range, but nephrotic-range proteinuria has been reported in a minority of cases. Serum albumin is usually better preserved, despite significant proteinuria, and a clinical nephrotic state is uncommon. Management of these patients is best offered by a multidisciplinary team consisting of a nutritionist, exercise trainer, nephrologist, and a specialist in lipid disorder. The strategy includes weight reduction, identification and treatment of risk factors for coronary heart disease, and treatment of hyperfiltration. She was the product of 37 weeks of gestation born via cesarean section, with a birth weight 9 lb. Pregnancy was complicated by maternal obesity, a 50-lb weight gain during pregnancy, and eclampsia, but there was no history of gestational diabetes in the mother. The patient was not breast fed and was advanced on formula and progressed by 4 months to rice cereal and onto solid foods in response to a "robust appetite. Review of systems was positive for gastrointestinal reflux disease and heavy snoring during sleep. She reports long-standing difficulty in keeping up with her peers in physical education. Urinalysis was negative for protein; the urine (micro) Insulin-sensitizing agents Metformin, a drug originally derived from the plant Galega officinalis, which had been used for treatment of diabetes mellitus, is also useful in the treatment of MetS. In effect, metformin increases tissue sensitivity to insulin and is also referred to as an insulin sensitizer. Thiazolidinediones, also known as glitazones (rosiglitazone and pioglitazone), are other types of clinically useful insulin sensitizers in MetS prediabetes management. Good glycemic control is essential in preventing nephropathy and other microvascular complications of diabetes. Unfortunately, these drugs have not been shown to forestall onset of nephropathy, when used as preventive agents in the early course of the disease. Hyperglycemia is masked by hyperinsulinism, but her 2-hour oral glucose tolerance test result is abnormal and the elevated HbA1c reflects suboptimal glucose regulation. Disordered sleep history is suggestive of obstructive sleep apnea that can aggravate insulin resistance. Although there is ample room for lifestyle improvements, this patient will need adjunct insulin-sensitizing and antihypertensive medications with intensive reinforcement of nutritional and activity changes. Type 2 diabetes among North American children and adolescents: An epidemiologic health perspective. Diabetic nephropathy in 27,805 children, adolescents, and adults with type 1 diabetes: Effect of diabetes duration, A1C, hypertension, dyslipidemia, diabetes onset, and sex. Urinary albumin excretion rate and glomerular filtration rate in the prediction of diabetic nephropathy: A longterm followup study of childhood onset type1 diabetic patients. Risk factors for early onset of diabetic nephropathy in pediatric type 1 diabetes. Higher prevalence of elevated albumin excretion in youth with type 2 than type 1 diabetes. Prevalence of diabetes complications in adolescents with type 2 compared with type 1 diabetes. Insulin signaling to the glomerular podocyte is critical for normal kidney function. Podocyte detachment and reduced glomerular capillary endothelial fenestration promote kidney disease in type 2 diabetic nephropathy. The case for intrarenal hypertension in the initiation and progression of diabetic and other glomerulopathies. Prevention of diabetic glomerulopathy by pharmacological amelioration of glomerular capillary hypertension. Kidney function in early diabetes: the tubular hypothesis of glomerular filtration. Genome-wide association scan for diabetic nephropathy susceptibility genes in type 1 diabetes. Replication study for the association between four loci identified by a genome-wide association study on European American subjects with type 1 diabetes and susceptibility to diabetic nephropathy in Japanese subjects with type 2 diabetes. Microalbuminuria predicts clinical proteinuria and early mortality in maturity-onset diabetes. Clinical practice guidelines and clinical practice recommendations for diabetes and chronic kidney disease. The significance of the prepubertal diabetes duration for the development of retinopathy and nephropathy in patients with type 1 diabetes. Risk of microalbuminuria and progression to macroalbuminuria in a cohort with childhood onset type 1 diabetes: Prospective observational study. Relationship between renal volume and increased albumin excretion rates in children and adolescents with type 1 diabetes mellitus. In patients with type 1 diabetes and new-onset microalbuminuria the development of advanced chronic kidney disease may not require progression to proteinuria. Adherence to clinical practice guidelines in the management of children, youth, and young adults with type 1 diabetes: A prospective population cohort study. Intensive glucose control improves kidney outcomes in patients with type 2 diabetes. Role of intensive glucose control in development of renal endpoints in type 2 diabetes: Systematic review and meta-analysis. Intensive glycemic control in type 2 diabetics at high cardiovascular risk: Do the benefits justify the risks Microalbuminuria and risk for cardiovascular disease: Analysis of potential mechanisms. Angiotensin converting enzyme inhibitor therapy to decrease microalbuminuria in normotensive children with insulin-dependent diabetes mellitus. Randomised placebocontrolled trial of lisinopril in normotensive patients with insulin dependent diabetes and normoalbuminuria or microalbuminuria. Should all patients with type 1 diabetes mellitus and microalbuminuria receive angiotensin-converting enzyme inhibitors Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. Effect of candesartan on microalbuminuria and albumin excretion rate in diabetes: Three randomized trials. The impact of reninangiotensinaldosterone system inhibitors on type 1 and type 2 diabetic patients with and without early diabetic nephropathy. Effect of dual blockade of the renin-angiotensin system on the progression of type 2 diabetic nephropathy: A randomized trial. Magnitude and determinants of coronary artery disease in juvenile-onset, insulin-dependent diabetes mellitus. Trends in allcause and cardiovascular disease mortality among women and men with and without diabetes mellitus in the Framingham Heart Study, 1950 to 2005. Cardiovascular and renal protection in type 2 diabetes mellitus: the role of calcium channel blockers. Definition, diagnosis and classification of diabetes mellitus and its complications. Geneva: World Health Organization, Department of Noncommunicable Disease Surveillance; 1999. Is waist-to-height ratio a useful indicator of cardio-metabolic risk in 6-10-year-old children Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Prevalence of a metabolic syndrome phenotype in adolescents: Findings from the third National Health and Nutrition Examination Survey, 1988-1994. Common familial influences on clustering of metabolic syndrome traits with central obesity and insulin resistance: the Kiel obesity prevention study. The search for putative unifying genetic factors for components of the metabolic syndrome. Genetics in endocrinology: Genetic forms of severe insulin resistance: What endocrinologists should know. The inflammatory syndrome: the role of adipose tissue cytokines in metabolic disorders linked to obesity. Major food sources of calories, added sugars, and saturated fat and their contribution to essential nutrient intakes in the U. Cardiovascular health behavior and health factor changes (1988-2008) and projections to 2020: Results from the National Health and Nutrition Examination Surveys. Childhood-adolescent obesity in the cardiorenal syndrome: Lessons from animal models. Morphometric and immunohistochemical insight into focal segmental glomerulosclerosis in obese and non-obese patients. Clinicopathological characteristics of obesity-associated focal segmental glomerulosclerosis. The effect of metformin and intensive lifestyle intervention on the metabolic syndrome: the Diabetes Prevention Program randomized trial. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. Metformin revisited: Re-evaluation of its properties and role in the pharmacopoeia of modern antidiabetic agents. Is there a rationale for angiotensin blockade in the management of obesity hypertension Statins and risk of incident diabetes: A collaborative meta-analysis of randomized statin trials. Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents.
Thyroxine 75 mcg order fast delivery. Pneumonia Home Remedies - Natural Ayurvedic Home Remedies For Pneumonia.
References
- Hudson PL, Thomas K, Trauer T, Remedios C, Clarke D. Psychological and social profi le of family caregivers on commencement of palliative care. J Pain Symptom Manage 2011;41(3):522-34.
- Rossi G, Cavazza A, Spagnolo P, et al. Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia syndrome. Eur Respir J 2016;47(6):1829-1841.
- Lacut K, Bressollee L, Le Gal G, et al: Prevention of venous thrombosis in patients with acute intracerebral hemorrhage, Neurology 65:865-869, 2005.
- Acetabular labrum: abnormal findings at MR imaging in asymptomatic hips. Radiology 216 (2), 576.
- Chopra S, Metcalfe C, Satkunasivam R, et al: Initial series of four-arm robotic completely intracorporeal ileal ureter, J Endourol 30:395, 2016.